
Date: Sun, 5 Mar 2000 12:51:10 EST
From: TR Toal Jr
Subject: Segmental tibia nonunion
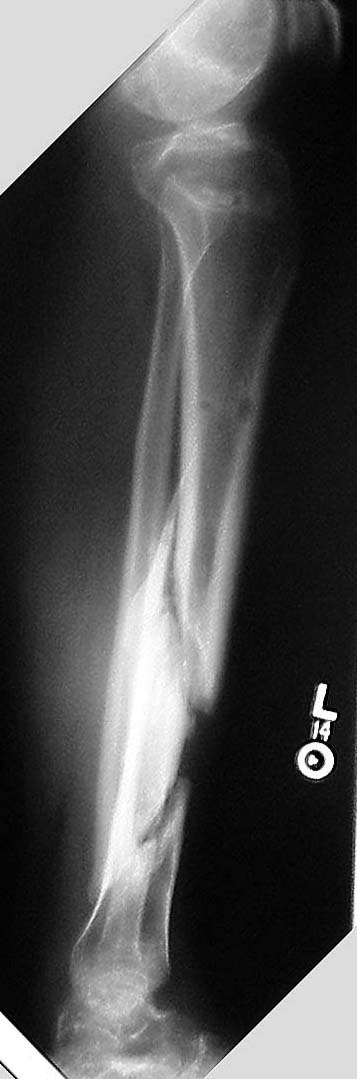
This 41 year old man, an ex-Olympic skiier, fell in 7/99 while traveling 120MPH on skis. He sustained several injuries which have healed uneventfully. His closed tibia fracture was treated initially with an Ilizarov frame at another hospital. He developed major fracture blistering, but no compartment syndrome. The frame became very loose without major pin tract infection, and was removed in 12/99. A PTB cast was placed and weight bearing encouraged. There is still gross motion at the distal fracture. A recent MRI and bone scan suggest that the segment is not avascular. Recent plain films are attached. Any suggestions?
Tom Toal
|
|
Date: Sun, 5 Mar 2000 17:04:14 -0500
From: bruce meinhard
The alignment of the tibia is good on both views. I would suggest that if infection is ruled out through ESR and CRP levels, biopsy for culture if you are really inquisitive, this would respond to a large reamed locked IM rod and bone graft. the success rate should exceed 90%.
BPM
Date: Mon, 6 Mar 2000 10:39:07 +0100
From: Fabrizio Margheritini
Actually I agree with Bruce suggesting an intramedullary blocked reamed nail plus a peroneal (fibular) osteotomy and bone grafting and I would suggest a white blood cells bone scan for ruling out infection without any doubts.
Fabrizio Margheritini
Date: Mon, 06 Mar 2000 10:40:26 -0600
From: Adam Starr
If you're in a gamblin kind of mood and the infectious indices are all normal, you could consider nailing it. I would do my darndest to nail it closed (I bet you still could) but be prepared to open it.
The other option is to place another ring fixator. If placed well, you could control all the major fragments and hopefully provide enough stability in time to allow full weight bearing. This is less risky than the nail, since you're not shoving a piece of metal into a potentially infected bone.
Still, if the guy came into my office with those xrays, and clean skin, and normal infectious indices, a nail is probably what I'd recommend.
Just my 2 cents.
Adam Starr
Date: Mon, 6 Mar 2000 7:17
From: Bill Burman
See comments on a worse case scenario presented by Tom DeCoster in 1995.
Since the alignment is acceptable, what about a plain old, non-metallic, relatively low risk, posterolateral bone graft plus or minus colagraft?
Furthermore, does anybody have any experience with an even less invasive method - marrow osteoprogenitor cells to stimulate osteogenesis as described by Connolly?
Bill Burman, HWB Foundation
Date: Mon, 6 Mar 2000 22:51:18 +0500
From: Alexander Chelnokov
Hello,
His closed tibia fracture was treated initially with an Ilizarov frame at another hospital.
Did you see images with that frame? Was reduction better than at presented images?
He developed major fracture blistering, but no compartment syndrome.
The injury was severe enough.
The frame became very loose without major pin tract infection,
The Ilizarov frame in cases like this is a real "plug and play" device, not "plug and forget". Routine control of stability is required during fixator in place such as maintenance of wire tension and wire/pin change in case of loosening.
There is still gross motion at the distal fracture. A recent MRI and bone scan suggest that the segment is not avascular.
I have nothing against closed interlocked nailing except i have never seen it in real life ;-( So if the patient would be here i would use the Ilizarov (with pins and wires) for the case. The fracture pattern seems to allow transverse compression as well as bone grafting, either conventional or percutaneous osteotomy and transport of sliding bone fragment to overlap one or both gaps. It seems to me though that proper ex-fix may be quite enough without grafting - it can become more clear after fixator application and gradual reduction.
Best regards, Alexander N. Chelnokov, Ural Scientific Institute of Traumatology and Orthopaedics 7, Bankovsky str. Ekaterinburg 620014 Russia
Date: Mon, 06 Mar 2000 11:56:41 -0600
From: Adam Starr
I have nothing against closed interlocked nailing except i have never seen it in real life ;-(
Well, man, we need to get you over to Dallas to visit!
Date: Mon, 6 Mar 2000 23:14:39 +0500
From: Alexander Chelnokov
Hello Bill,
Monday, March 06, 2000, 6:46:31 PM, you wrote:
BB>See comments on a worse case scenario presented by Tom DeCoster in 1995
Yes, i remember that extremely severe case. And that discussion IMHO was a good example of real telemedicine.
BB> Furthermore, does anybody have any experience with an even less invasive BB> methods - e.g. marrow osteoprogenitor cells to stimulate osteogenesis
IMHO all these non-invasive methodics (electromagnetic fields, ultrasound, stem cells and so on) are not too harmful if applied not solely but along with perfect surgical treatment.
Best regards, Alexander N. Chelnokov, Ural Scientific Institute of Traumatology and Orthopaedics 7, Bankovsky str. Ekaterinburg 620014 Russia
Date: Mon, 6 Mar 2000 16:00:40 -0500
From: bruce meinhard
does anybody have any experience with an even less invasive methods
I have used the injection of bone marrow aspirate mixed with Grafton for adjunctive treatment in anticipated delayed nonunions and have a 50% anecdotal success with this method.
BPM
Date: Mon, 06 Mar 2000 13:48:36 -0700
From: Thomas A. DeCoster M.D.
Regarding the 1995 case. I will try again to post a recent radiograph. It eventually healed with a "saved" leg and union of all 37 tibial pieces to each other. I used ring fixator in various configurations. The patient is walking on the leg with skin and bone healed and glad he went through the 2 years of treatment versus early amputation.
That said, in the currently posted case I would suggest IM nailing, perhaps in 2 stages with the first stage to reduce the risk of infection. The "avascular" segment may very well revascularize if the leg is stabilized with a nail he can be walking on it during the months it will take to revascularize and heal.
Tom DeCoster
Date: Tue, 7 Mar 2000 21:46:55 -0600
From: Anglen, Jeffrey
Bill - Thanks for including the electronic references regarding less invasive treatments for nonunion. We all like to operate, sometimes too much. I am as guilty of that as anyone.
Having just finished reviewing the topic of bone stimulators for a talk at the OTA's trauma update course in Kansas City (which, by the way I hope you are all aware of and encouraging the orthopods in your community to attend) I have become convinced that they work! There is far better science (double blind, prospective, randomized trials) demonstrating effectiveness of electromagnetic and ultrasonic bone stimulation than there is for bone grafting, nailing, external fixation or any surgical treatment. Essentially every comparison shows stimulation to be equal to or better than surgery, especially when surgery has failed once.
I have attached for your information a copy of the annotated bibliography I put together for that talk. In exchange, I hope everyone will help promote the OTA's Trauma Update course by telling your partners, referring docs and friends about it. Did I mention that already? See the OTA web page for details.
Thanks -
Jeff
Date: Wed, 8 Mar 2000 09:02:31 -0600
Forwarded message from: Ray White
I rarely reply to these forums, but I here I go. If this guy is an ex-olympic skiier, he will not stop and he must be perfect rotationally to ski. Fracture is low for a nail and very complex to get the nail across both sites.
I would resort to the gold standard for nonunions: Compression Plating!
Date: Wed, 08 Mar 2000 10:00:04 -0500
From: Langdon Hartsock
I agree with Ray. If soft tissues are good then Lag fixation with neutralization plate and bone graft as necessary would be my first choice.
Langdon A. Hartsock, MD, Medical University of S. Carolina, Charleston, SC
Date: Wed, 8 Mar 2000 19:03:13 -0000
From: Chris Wilson
Could I add that we have used the Exogen Ultrasonic system (Smith & Nephew here in the UK) on 4 nonunions of tibia and femur with 100% union rate at 6 months after commencing treatment. Small numbers but a very useful device, especially with a severe and unforgiving fracture like the one under discussion.
Regards
Chris Wilson, Orthopaedic Surgeon, University Hospital, Cardiff, UK
Date: Wed, 8 Mar 2000 17:17
From: Bill Burman
Two tibial ultrasound papers were presented at the 1999 OTA Annual Meeting.
Bill Burman, HWB Foundation
Date: Wed, 08 Mar 2000 17:16:46 -0600
From: Steven Rabin
i don't look at my email for a few days and it fills up! mostly i agree with the options everyone else has mentioned but i'll throw in my two bits too.
i would do a closed reamed rodding with fibular osteotomy possibly with ultrasound or e-stim (noninvasive) postop. Cultures from the canal and reamings would help and be sure that your lab takes staph epi. seriously. this looks like a relatively atrophic nonunion and a low grade infection needs to be a concern. i would rod it even if i found pus as the stability would encourage healing and the reaming could help debride the medulllary canal. if it is infected, plan on eventually removing the rod.
i think this can be rodded closed. have available sharp reamers and flexible hand reamers and even flexible enders rods if necessary to get past the fracture sites if they are sclerotic and closed off. the advantage of the closed rodding is that he can be weightbearing and using the leg fully almost immediately.
i would not do an external fixator as he had problems with a fixator for whatever reason before and patients tend not to be full weightbearing with them if they have any pin problems.
Plating would require a much longer open incision as i think you would have to span both fracture sites and if his bone quality is poor it may be awhile before you can let him be full weightbearing. Also if it is infected, plates do less well and may loosen faster than the rod. If i did plate it, i would consider an implanted electrical stimulator plus bone graft.
the trouble with plating in an obsessive world-class skier is that he will ski again and his next injury could be a peri-implant fracture at the end of the plate. And if we ever take the plate out, will he ski again too soon and rebreak through the old fractures? i'd be more comfortable letting him ski with a rod that protects the whole bone with less stress shielding than with the plate.
A "simple" posterolateral bone graft is a possiblitity but the segmental fragment is probably somewhat avascular despite the mri report and i would think it would take longer to heal and he'd need to be in some sort of brace or other immobilization for a longer period of time than if you went straight to the rodding.