



Date: Mon, 23 Jun 2003 20:17:38 -0700
Subject: Tibial defect
Need some group input on this one...
45 year old healthy non-smoker is six weeks post type 3B open tibial fracture. Latissimus flap looks perfect. Tibia is about 20 degrees externally rotated and in valgus. Intact pulses and sensation. Defect is 10-11 cm.
|
|
|
|
Transferred to my care today.
I'd love to nail and graft this one, rather than starting a 9 month Ilizarov lengthening.
Is it too big to nail and graft?
Does this require a bifocal lengthening?
Tom Toal
Portland, Oregon
Date: Tue, 24 Jun 2003 11:21:17 +0600
From: Alexander Chelnokov
Hello Tom,
TT> I'd love to nail and graft this one, rather than starting a 9 month Ilizarov lengthening.
Why not perform nailing immediately after docking?
Best regards,
Date: Tue, 24 Jun 2003 16:26:17 +0530
From: DR T I GEORGE
Dear Tom Toal,
I would keep open the following options depending on expertise and facilities available locally.
1) Removal external fixator, interlocking nailing using a solid nail. Then bridge the defect using a microvascular free fibular transfer.
2) Microvascular fibular transfer along with augumentation of external fixator. Conversion to a ring fixator may be the best for stability till the graft consolidates.
3) Nailing with bone transport over the nail.
4) Change to Ring fixator with bone transport to bridge the graft.(Bifocal would diminish time duration.)
Using the imagination, various options like trasferring the same uppr fibula to the defect as a pedicled graft with augumentation of the fixator etc can also be tried in this difficult situation.
Will be happy to know how you have tackled this difficult problem.
Best of luck.
Date: Tue, 24 Jun 2003 07:41:30 -0700
From: Chip Routt
Here's one that we've shown this list before...this patient consolidated his defect with a single allo/auto combination direct defect grafting @ 6 weeks.
It's anecdotal, but can work-
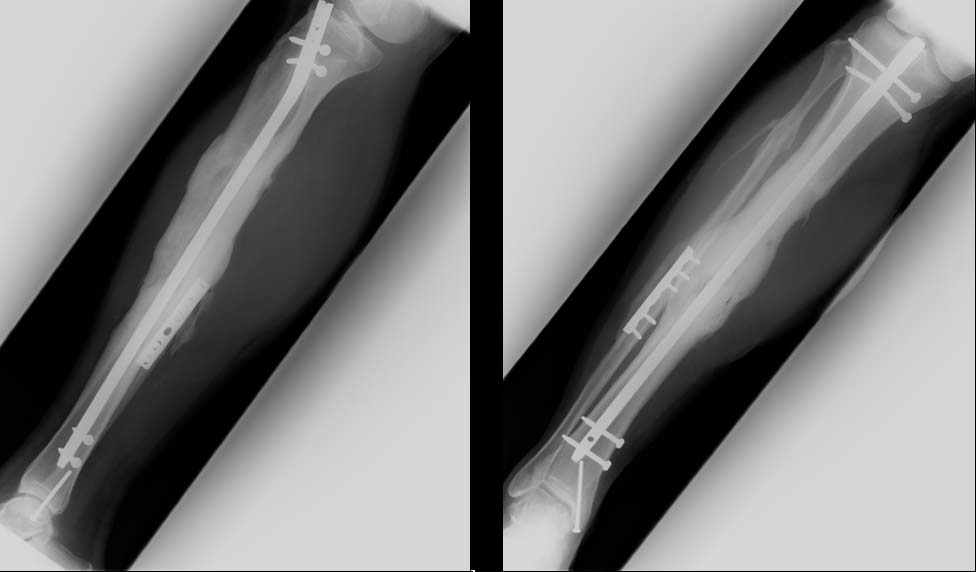 |
Date: Tue, 24 Jun 2003 11:15:24 -0500
From: Obremskey, William T
Big defect, but if no active or history of pin tract infection, I think it is reasonable to remove fixator, align, IMN and huge graft as Chip demonstrated can work.
Attached are some references that might be useful for exchange IMN and large defects.
Date: Thu, 26 Jun 2003 14:35:25 -0600
From: Thomas A. DeCoster
I think bone transport is the best treatment in this situation. It offers the best chance of successful limb salvage and function, although it will likely take a long time (12 months). Bifocal transport can work but depends upon fracture location and bone availability at both ends. IM nail after transport might shorten consolidation/healing phase. IM nail and bone graft now is simpler at first but seems unlikely to reliably fill that large of defect. It could be part of staged treatment.
Other options: I don't think bone graft alone will work very well. With previous free flap, another vessel for free fibula seems unlikely plus other problems.
Bone graft substitutes not potent enough for this big gap. Structural allograft has big risk of infection.
Tom DeCoster
Date: Sat, 28 Jun 2003 13:15:19 +0600
From: Alexander Chelnokov
Hello Chip and all,
CR> Here's one that we've shown this list before...this patient consolidated his CR> defect with a single allo/auto combination direct defect grafting @ 6 weeks.
BTW what finally was done to the patient discussed in March 2003 with similar defect presented by Thomas Higgins?
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Sat, 28 Jun 2003 03:22:03 -0700
From: solon.rosenblatt
A way to treat the tibia is what we were doing with Ron Lindsey in Houston up until I left; put a titanium cage measured for the size of the defect, pack it with autologous bone and bmp, chicken soup and whatever and then put a small reamed IM rod down. Close it up and hope it incorporates. I don't have much follow up on the technique. We did six and five of them are still doing well, five years later, but it takes forever for the bone to incorporate.
Solon