


Date: Mon, 27 Dec 2004 17:10:42 +0100
From: Dr. Josep M. Muñoz Vives
Subject: Open Pelvic Fracture
I would like some help with this patient.
He is a 30 yo male that 2 weeks ago was caught in a building in flames. He and other 4 people jumped from different heights because the fire was approaching. He has 2nd degree burns in both legs (<5% body surface).
He arrived to our hospital with the following injuries:
A) Awake and alert. No great hemodynamic instability.
B) Mild right pneumotorax
C) L1 fracture
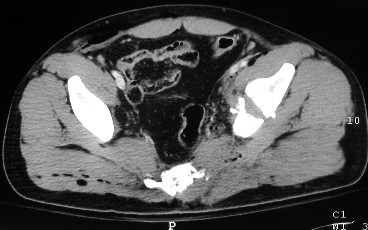
D) Anterior column and posterior hemitransverse of the left acetabulum (62-B3.2)
E) Pubic symphysis diastasis (61-C1.1)
F) Sciatic spine arrachment
G) Left perineal wound Didn' t arrive to the pelvic cavity.
H) Right gluteal wound. The wound arrived to the presacral space, but the rectal fascia was not injured. The function of his sciatic nerve is normal, as the continence of the anal sphincter.- You can see some air in the obturatus muscle.
|
|
|
 |
 |
 |
A right chest tube, urethral catheter, femoral skeletal traction and antibiotics were placed. He has been given 5 units of packed red cells. The gluteal and perineal wounds were debrided
The course of the perineal wound has been good. Beginning in the fourth day purulent discharge has ensued in the gluteal wound and the temperature rose to 38ºC
 |
 |
 |
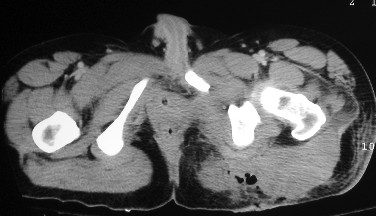 |
On the 7th day we practiced a new CT. There was a collection emerging from the gluteal wound that extended subcutaneously to the 3rd lumbar vertebra with air inside the, so we decided to wash it with pulsate lavage and drain it.
The purulent discharge continued so we decided to debride him again. Plenty of necrotic tissue was found (which was removed). But today the communication to inside of the pelvis was macroscopically closed.
He has got a polymicrobian infection.(Enterobacter, E. coli, Staphylococcus grew in the cultures) and we are treating him with ciprofloxacin and amikacin.
 |
 |
Taking care of the wound with him awake is a real problem. The wound and the Morel-Lavalle are on his back, so we have to roll him or elevate him with a crane. He is in a lot of pain even though we give him morphine when we move him.
 |
 |
 |
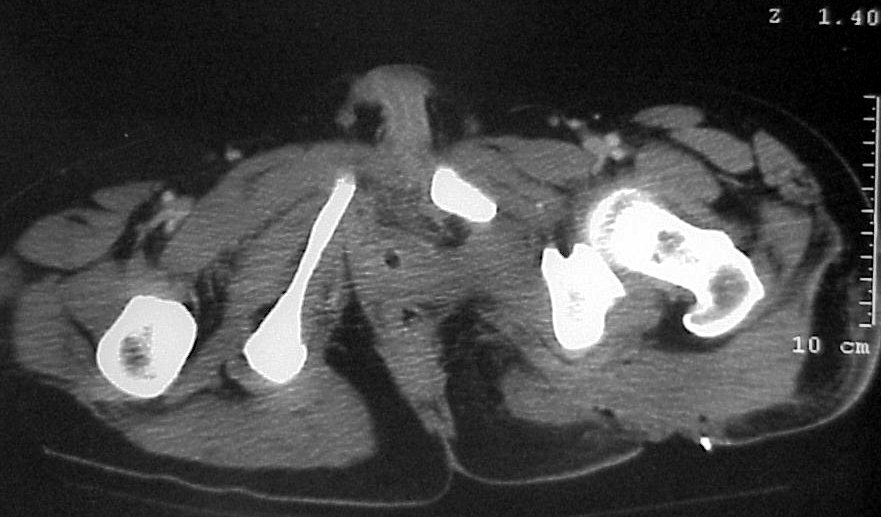 |
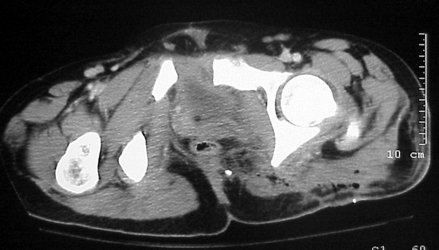
We performed another CT yesterday and look for any sign of persistent infection inside the pelvis. Our radiologist say that it seems that the infected cavity in his back does not communicate with the inside of the pelvis. Our plan is to fix the anterior part of the fracture through an ilioinguinal approach. We think that this will help a lot in the management of the patient, allowing us to roll him with less pain.
What are your thoughts?
Thanks in advance.
Dr. Josep M. Muñoz Vives
Orthopedic Dept.
Hospital Universitari Dr. Josep Trueta.
Girona
Catalunya, Spain
Date: Mon, 27 Dec 2004 11:29:51 -0800
From: Chip Routt
Some might call it an associated both column fracture pattern based on the submitted images, but you've seen the 2D axial images.
Regardless of the pattern, I agree to reduce and fix the acetabular and symphyseal injuries using the ilioinguinal exposure.
The reduction will be a bit more difficult at 2 weeks, especially for the posterior column component.
His open wound management is greatly improved if his acetabular and symphyseal injuries are reduced and stabilized.
Some believe that infection rates are decreased with osseus and resultant soft tissue stability.
A perfect reduction should seal his hip joint from further exposures.
Chip