
Date: Date: Thu, 12 Jun 2003 21:12:45 +0200
From: Josep M. Muñoz Vives
Subject: Floating knee
This 48 yo male suffered a motorbike accident 4 days ago.
- Mesocolon tear needed a laparotomy to control.
- Nondisplaced fracture of the posterior acetabular lip
- Grade IIIA open fracture of the left femur (33-C3.3) whith a 15 cm wound on the anteromedial region of the femur
- Grade IIIA open fracture of the left tibia izquierda (41-C3.35)
|
On day of admission debridement and lavage of the fracture was performed. An anterior external fixator was applied.
Now the patient and its wounds look fine.
Any suggestion will be welcomed
Dr. Josep M. Muñoz Vives
Orthopedic Dept.
Hospital Universitari Dr. Josep Trueta.
Girona
Catalunya, Spain
Date: Fri, 13 Jun 2003 01:21:45 +0530
From: DR T I GEORGE
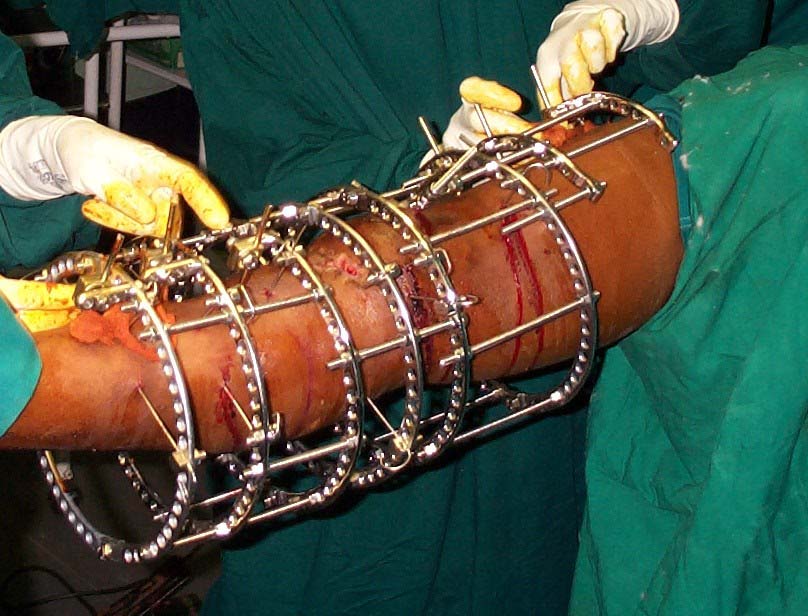
Suggest a ring fixator. I am attaching pictures of a similar case treated with ring fixators after the soft tissues settled down.
 |
 |
 |
 |
 |
DR T I GEORGE
Head of Orthopaedics Unit III
Little Flower Hospital
Angamaly, Kerala State, India.
Date: Fri, 13 Jun 2003 09:35:40 +0300
From: Anton V. Vladzimirskyy
Hard case! I have similar one. 1) Best way - open reduction and external fixation (by Ilizarov frame). No more function (only rocking), but good bone and soft tissue reparation. 2) Massive antibiotics therapy, intrajoint lavage (2-4 days) with antiseptic fluid
Best wishes,
dr. Anton Vladzymyrskyy M.D.
Department of Polytrauma
R&D Institute of Traumatology and Orthopedy
Donetsk, Ukraine
Date: Sat, 14 Jun 2003 07:46:50 EDT
From: Aobonedoc
Having reviewed the xrays, IM rod of tibia not possible.
Possible retrograde nailing of femur, lag screws to distally secure condyles may be needed. Perhaps Synthes LIS fixation but I have never used this.
Tibia probably needs ex fix. I might consider implantation of antibioitic calcium sulfate beads although I have not done this in the acute setting of open fractures (just treatment of osteomyelitis).
Good luck. Total knee someday.
Sincerely and respectively,
Date: Fri, 27 Jun 2003 15:44:36 +0200
From: Josep M. Muoz Vives
The patient I posted two weeks ago was operated last week. We used 2 LISS plates.
Articular surfaces and axis looks acceptable but the patient left his tibial tuberosity in the road. The patellar ligament is severed level with its insertion on the tibia and there is no tibial tuberosity. I used two sutures and anchored the patellar ligament to the tibial LISS screws but it is floating in the middle of a gap.
 |
 |
What do you recommend as next move?
Dr. Josep M. Muñoz Vives
Orthopedic Dept.
Hospital Universitari Dr. Josep Trueta.
Girona
Catalunya, Spain
Date: Fri, 27 Jun 2003 19:30:31 +0100
From: Chris Wilson
In a similar scenario I have used semitendinosis and gracilis tendons, stripped as in an anterior cruciate ligament reconstruction,and left attached distally, and threaded proximally through a transverse tunnel through the lower half of the patella, and brought distally again to be sutured alongside the tendon attachment, in a loop, and the free ends placed in a cancellous bone trough in the tibial tubercle and secured with an AO screw and washer.
It is described for patella tendon rupture in TKA, and I have done this in 2 patients in similar situations to yours, with a functioning extensor mechanism at 6 months and 18 months, with slight extensor lag in both cases. We didn't write it up as we didn't think it was novel enough, but the strength of the 4 strand hamstring is enough to function as a patellar tendon. Brace in full extension for 6 weeks and avoid resisted extension and loaded flexion for 3 months. (based on bone ingrowth and tendon weakening data from ACL reconstruction.)
Regards
Chris Wilson
Knee and Trauma Surgeon
University Hospital
Cardiff, UK