

Date: Wed, 27 Jun 2001 20:00:36 -0600
Subject: Pediatric Subtrochanteric Femur Fx
From: Kanlic, Enes M. M.D.
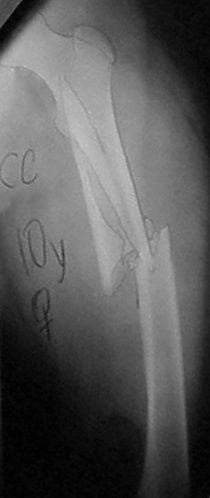
Regarding pediatric femur fractures, I am wondering how would the members address this comminuted subtrochanteric fracture in 9 years old girl, 34 kg weight, with opposite tibial spine avulsion in stable medical condition?
|
|
|
Enes M. Kanlic, MD, PhD
TTUHSC Ortho Dept
El Paso, Texas
Date: Wed, 27 Jun 2001 23:32:05 -0500
From: Adam Starr
After our discussion, this seems like a great case for one of those pedi nails with a trochanteric entry point. I wonder if the pedi nails allow placement of locking screws up into the neck?
But, I bet your technique of percutaneous plating could be used, too. Maybe angle some screws up into the neck?
As Roy Sanders said earlier, there are folks who are "magicians" with Enders' nails. I'm sure some would use Enders' on this fracture.
Is this one you've already treated, or a new case?
Adam Starr
Dallas, Texas
Date: Thu, 28 Jun 2001 05:13:06 -0700
From: bruce meinhard
Off-brand use of the AO tibial rod inserted antegrade through the greater trochanter as described by Brumbach et. al Plate or ex fix as alternatives.
bpm
Date: Thu, 28 Jun 2001 14:03:00 -0700
From: Carlo Bellabarba
perc plate.
carlo bellabarba
seattle
Date: Thu, 28 Jun 2001 19:31:03 -0400
From: Charles Mehlman
Early in my learning curve with Nancy Nails (6 years ago)- this type of subtroch fx bugged me and I even put a couple such kids in 90-90 traction followed by spica casting...
But now I feel almost as strongly that this is a great fracture to "fix" with Nancy Nails - probably 3.5 mm or 4.0 mm nails x two. I would cheat my nails as far as possible into prox fragment without violating growth plate. I would also not hesitate to add a least a "one-leg-spica" due to the comminution.
I would do such a case on a radiolucent (Jackson table) and then probably fix the tibial spine through a small arthrotomy at the same sitting.
Charles T Mehlman, DO, MPH
Assistant Professor Pediatric Orthopaedic Surgery
Division of Pediatric Orthopaedic Surgery
Children's Hospital Medical Center Cincinnati
Cincinnati, Ohio
Date: Thu, 28 Jun 2001 06:43:14 -0700
From: Chip Routt
EMK-
Preoperatively, you might enjoy improved/additional images of the proximal femoral fracture fragment.
Oblique (with traction) plain radiographs or several axial CT images will define the potential unrecognized trochanteric fracture components, which could in turn have adverse impact on your selected technique.
Thanks-
Chip Routt, M.D.
Harborview Medical Center
Seattle, Washington
Date: Thu, 28 Jun 2001 08:07:51 -0600
From: Kanlic, Enes M. M.D.
Chip R.,
Unfortunately, I have not digitalize the posted x-rays perfect. My intention was not to trick anybody, I was pretty sure that we have what I have described - comminuted subtrochanteric fx not involving trochanteric region. Also, in my operating room I have always all options available in case that I have to switch the gears.
Adam,
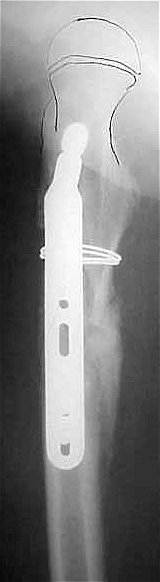
This is a done case. I thought that trochanteric entry point is potentially too risky (see Ch. Mehlman and my discussion from before). Bridge plate with screws going into the neck is definitively the option (as you can see it from this case with fx extended proximally to the lesser trochanter, the first one which I have done for pediatric femur fractures).
 |
 |
 |
Let see if we have some other suggestions, thanks for your responses.
Enes M. Kanlic, MD, PhD
TTUHSC Ortho Dept
El Paso, Texas
Date: Thu, 28 Jun 2001 19:34:40 -0400
From: Charles Mehlman
Nice images.
Nice clincial photo.
Great job of "bypass plating".
Very bio-logical.
Charles T Mehlman, DO, MPH
Assistant Professor Pediatric Orthopaedic Surgery
Division of Pediatric Orthopaedic Surgery
Children's Hospital Medical Center Cincinnati
Date: Thu, 28 Jun 2001 16:34:21 -0700
From: Chip Routt
EMK-
No trick anticipated.
The best time to "switch gears" is PRE-operatively, during a planning session based on complete information.
These recommended radiographic images alert the treating surgeon to potential problems PRE-operatively, facilitating a strategic plan, and avoiding a variety of adverse INTRA-operative "situations".
Chip
Date: Thu, 28 Jun 2001 19:57:52 -0600
From: Kanlic, Enes M. M.D.
O.K. Chip,
We got the point. Tell me please, how would you fix this fracture.
EMK
Date: Fri, 29 Jun 2001 07:17:20 -0700
From: Chip Routt
EMK-
If the CT demonstrated the proximal fragment to be without secondary fractures, I'd choose plating, framing, or nailing depending on soft tissue exam, other injuries, clinical condition, patient/limb size, parental discussion, among other factors.
I'm not emotionally or otherwise restricted to any one technique for fracture management. Each method has advantages and disadvantages. I'd discuss these options and details with the patient's parents.
That's about it, thanks-
Chip
Date: Fri, 29 Jun 2001 08:54:04 -0600
From: Kanlic, Enes M. M.D.
Chip R.,
That is nice, but patients usually ask me what is my recommendation and what is my first choice.
In this particular case, my
 |
 |
 |
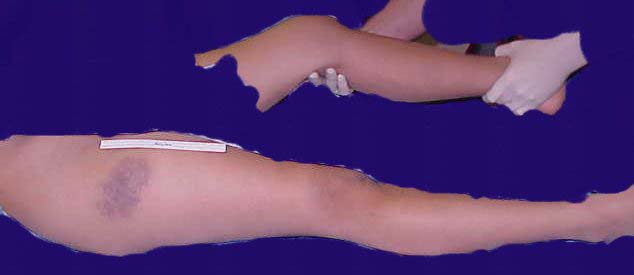
This patient had 110 degrees hip dynamic screw put in (regular, flat radiolucent table). Although I felt necessary to put the cerclage wire for better reduction, that was done with minimal additional damage and I would still consider it as "bridge plating technique" (the scar length is not crucial determining factor). She was weight bearing as tolerated after 6 weeks (without crutches) and x-rays presented here are after 8 weeks.
On the L knee we did mini arthrotomy and tibial spine fixation with nonabsorbable suture (attachments can not be more than 75 kb, that why I can not show you all images).
Our group has more than 40 cases of bridge plating technique, hopefully we will present it at next year Academy meeting, and publish it after that. There are few more interesting cases, and if it is burning desire there to discuss it, I could post them as well.
Thanks for your responses and interesting discussions.
Enes M. Kanlic, MD, PhD
TTUHSC Ortho Dept
El Paso, Texas