


Subject: Tibial Malunion & Medial Knee OA
Date: Thu, 1 Nov 2001 11:11:17 +0200
From: Alo Kullerkann
Dear members,
I would like to ask your advice in the following case:
53 y/o male, had trauma 20 years ago. Now has tibial diaphysis malunion of 12 degrees varus and 14 deg. of retroversion. At present the problem is knee medial compartment osteoarthrosis due tibial malposition. What would you do in this case?
What is your pick and what type of fixation would you use? Your opinion is requested, surgery is planed in monday Nov 5.
Kind regards,
Alo
Alo Kullerkann, MD
Orthopaedic Resident
Mustame Hospital, Tallinn, Estonia
|
|
|
Date: Thu, 01 Nov 2001 10:23:18 +0000
From: b.meinhard
Metaphyseal corticotomy and ex fix with gradual correction ( Heidelberg Fixator is one option or Ilizarov apparatus a second). This permits any degree of correction in 2 planes and permits good healing potential.
bpm
Date: Thu, 01 Nov 2001 11:26:46 -0600
From: Steven Rabin
I'd do just the diaphyseal osteotomy, and use the oblique osteotomy technique to correct in all planes of deformity. If you do both osteotomies at once, you have to worry about both healing and i think it would be technically harder to be precise in the correction. if you do just the proximal osteotomy, you'd create a Z shaped bone which might make it technically more difficult to properly align a future total knee replacment or treat any future fracture. If the osteotomy by itself doesn't work, you can later do the high tibial osteotomy in a standard way knowing that you have a straight leg for any future problem. If the shaft osteotomy by itself works, you've saved the patient the additional morbidity of the combined procedures.
Date: Thu, 1 Nov 2001 20:27:43 +0200 (EET)
From: Alo Kullerkann
> i'd do just the diaphyseal osteotomy, and use the oblique osteotomy technique to correct in all planes of deformity.
Dear Steven,
What would be your choice of implant to fixate osteotomy?
Alo Kullerkann, MD
Orthopaedic Resident
Mustame Hospital, Tallinn, Estonia
Date: Thu, 01 Nov 2001 12:49:03 -0600
From: Steven Rabin
In general, i would be prepared preoperatively to do either rod or plate and base the decision on how well i was able to line up the medullary canal intraoperatively. Since i don't see any translation deformity, i think it probably can be rodded. (preoperative templating may be very helpful in knowing preop what you'd like to do but may be misleading since the deformity is in two planes.) I like a rod here because you can let him up full weight bearing almost immediately. However, a rod has the disadvantages of not allowing interfragmentary compression and if he does need a later treatment for the arthritis, it will be in the way of either later proximal tibial osteotomy or knee replacment and have to be removed. The advantages of plate technique include the ability to achieve interfragmentary compression with a lag screw outside the plate and the hardware is away from any anticipated later surgery. The disadvantage is that I usually don't allow weight-bearing for about 10 weeks (although I would allow early range of motion), and it requires much more soft tissue stripping. Roy Sanders described use of the plate in his description of the oblique osteotomy which was in JBJS a few years back.
I think in his case because further surgery may be needed, my first choice would be plate technique. Of course, try to do it as atraumatically as possible for the soft tissues to preserve periosteal blood supply. (I usually do the osteotomy similar to a corticotomy for Ilizarov procedures trying to minimize disruption of soft tissue attachments.)
Good luck.
steve rabin
Date: Thu, 1 Nov 2001 21:30:01 -0000
From: chris wilson
This man is 53 with knee pain.
All respondents so far have opined that the malunion should be corrected at the diaphysial level.
The chances of delayed or non-union of a diaphyseal osteotomy are significant.
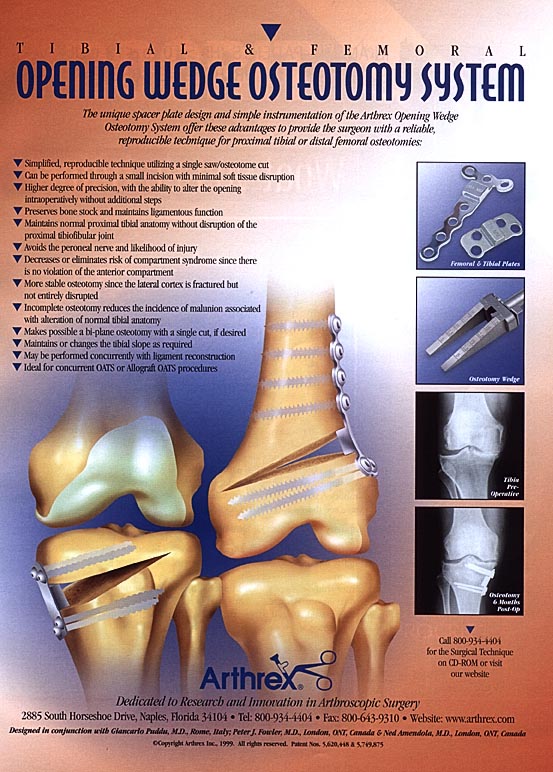
Given that the aim should be to align the whole tibia along the correct mechanical axis,with the ankle parallel to the transverse plane of the knee joint, my approach would be to perform an opening wedge high tibial valgus osteotomy, with sufficient correction to match the anatomical(as measured extramedullary) and mechanical axes, and with slight overcorrection.
I would use an "Arthrex" HTO plate (with a little attached wedge to support the osteotomy) and tricortical bone graft. This would give an overall correct alignment and avoid the need for second osteotomy. The deformity in the sagital plane can be ignored.
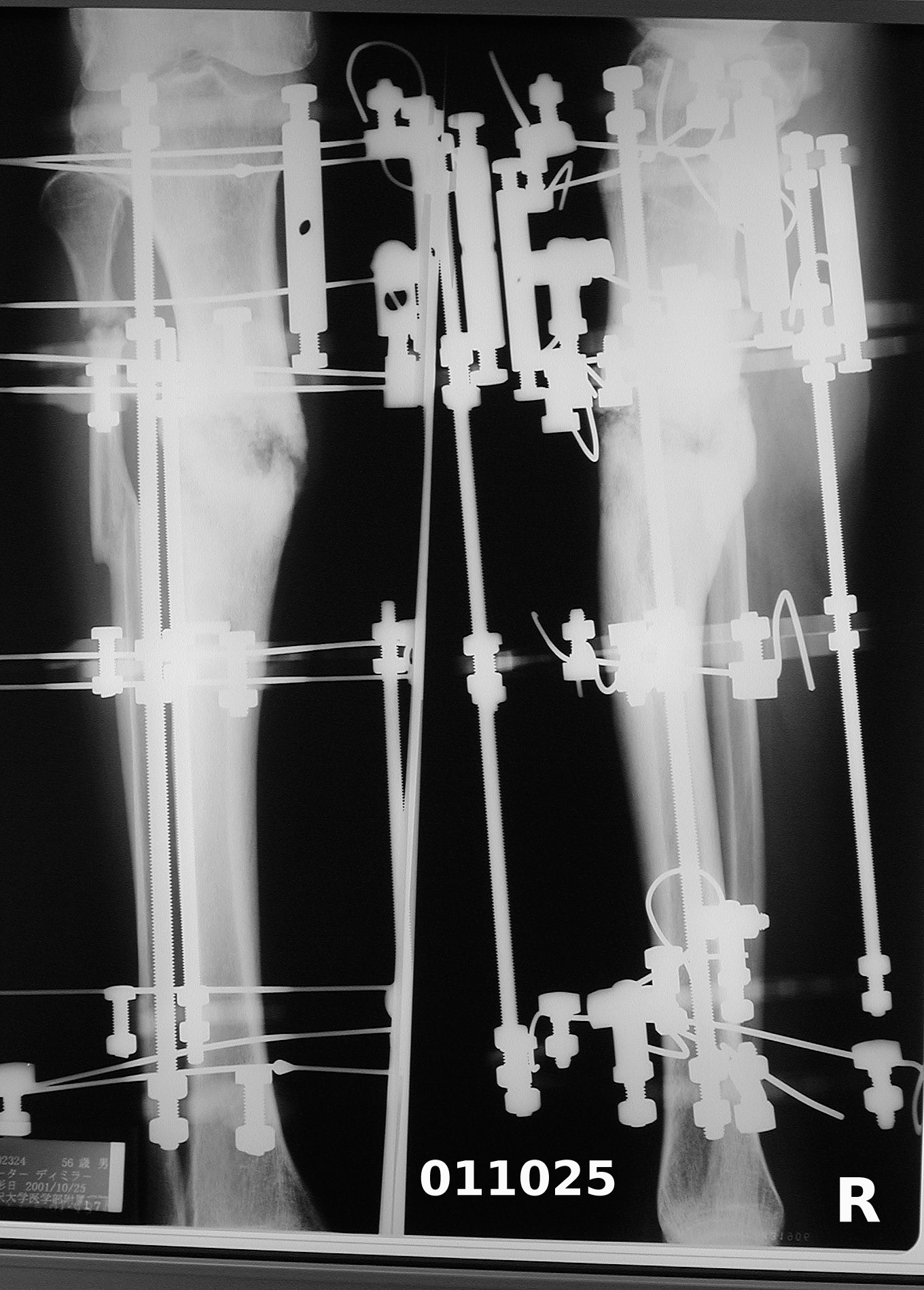 |
The case just reported by Dr Kullerkann (varus deformity of upper tibia originating from trauma 20 years previously, and similar age) seems remarkably similar to mine. While I cannot offer a medical opinion on which method would be best for that case, perhaps my case can serve as useful data. One respondent mentioned ex-fix, and as a patient I can report that this method seems to be successful in my case. The length of time required in my case is related to vascular damage from the 1971 trauma. I am looking forward to my right tibia being in better shape than it has been for 30 years.
With best regards,
Peter Miller
Kamakura, Japan
Date: Sat, 3 Nov 2001 16:31:19 -0000
From: Nuno Craveiro Lopes
Dear Alo,
As you described, you have a double deformity: one at the level of the malunitted fracture and a second one, secondary to the previous one, at proximal tibia. To get a good axis correction without a secondary Z deformity, which is important to prepare this limb for a future TKP, you must do a two level correction: One at the mid diaphyseal zone, including the axial on the plane of deformity and any shortening the patient can have, and the other at proximal tibia, with a 5-8 deg valgus overcorrection to decompress the medial compartment.
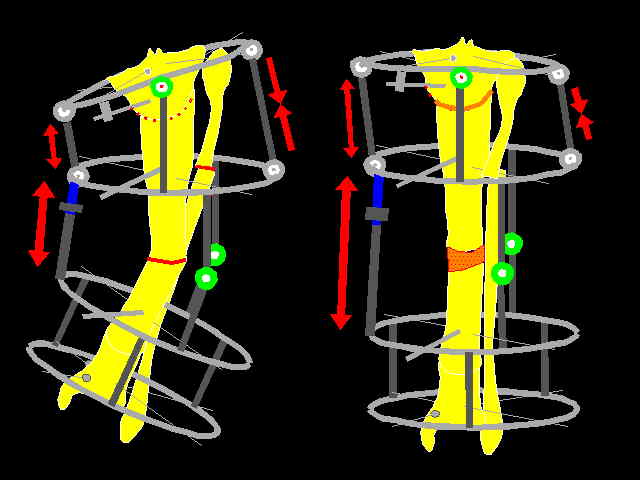 |
I suggest to do both corrections, the proximal with a curved osteotomy centred on the CORA and the diaphyseal at the deformity level, stabilising it with a Ilizarov frame and doing an acute correction if there are no shortening or progressive correction of the diaphyseal level if there is shortening as on the attached file.
Best regards,
Nuno Craveiro Lopes
Almada, Portugal
{kind=link}