

Subject: Re: Osteotomy for varus deformity of tibia
Date: Fri, 20 Oct 2000 18:43:27 +0900
From: Peter Miller
As a new subscriber, I would like to present a brief case summary and request information about suitable options. The case is my own. I understand that the list cannot substitute for a consultation. It might provide some enlightenment, however, not only to me, but to others who wish to follow what has so far proved to be a particularly challenging case.
|
|
|
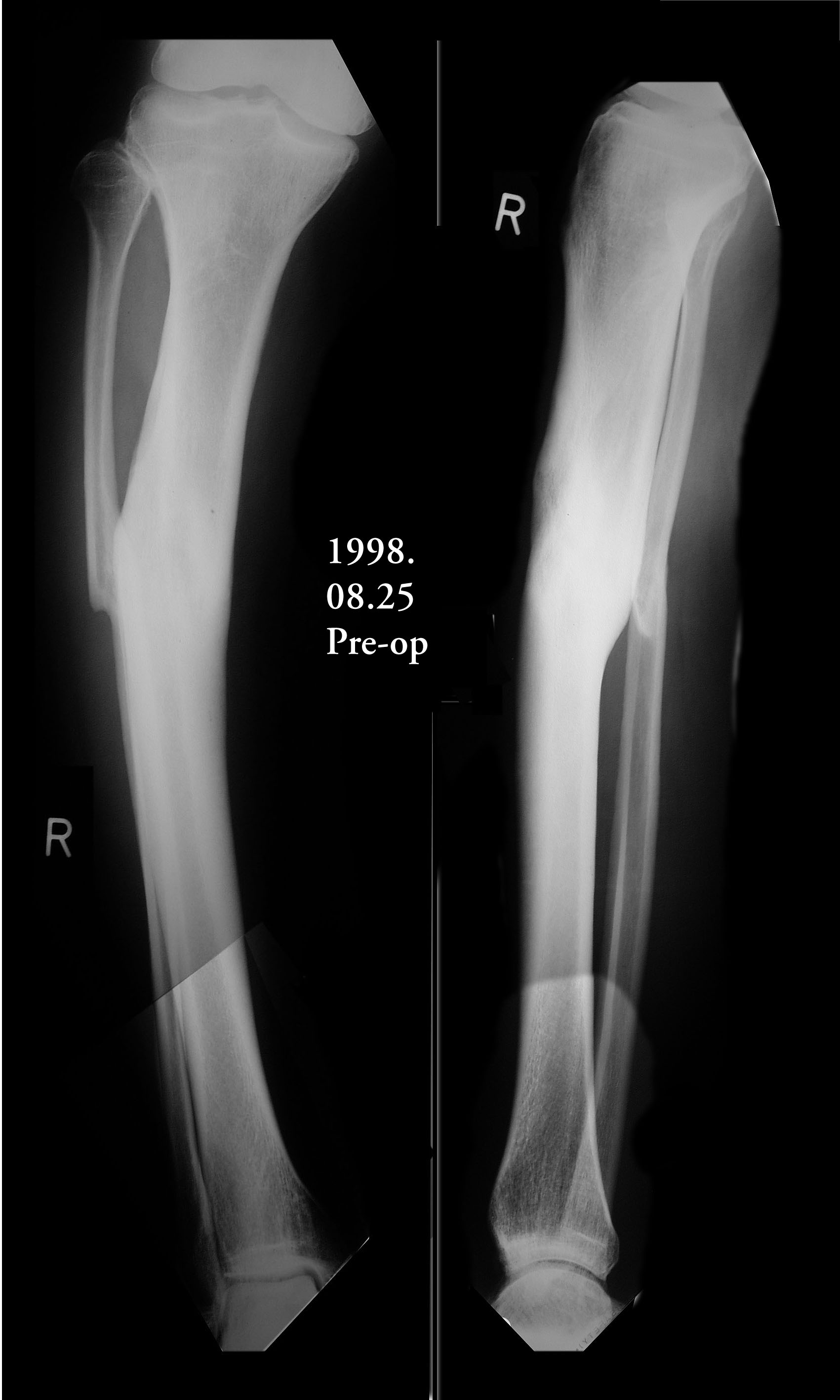
I am a 55-year-old male who suffered a compound fracture of the right tibia and fibula and extensive soft tissue damage, including vascular damage, from the impact of an automobile pinning the leg to a concrete wall in 1971. This occurred while I was a pedestrian. Emergency surgery restored circulation and set the tibia and fibula fragments with no internal fixation (due to concern about infection) and plaster cast immobilization. Later a bone graft was performed, and after physical therapy an apparently full recovery occurred, except a slight varus deformity, reduced vascularity, and reduced range of motion in the ankle. Over the years, the varus deformity worsened to 22 degrees and led to moderate osteoarthritis. To correct the deformity and straighten the tibia, an open-wedge osteotomy was performed in November 1999, with a bone graft from the other iliac crest. Plate fixation was used, as the bone was too hard to ream, so it was impossible to insert a pin. I have used the Exogen ultra-sound device every day since the surgery. Gradual improvement led to enhanced weight-bearing ability, and I have been walking with a cane since April 2000. Although X-rays taken June 16 showed no deformity, the varus deformity has recurred in the October 16 X-rays.
I am interested in why this happened and what to do about it. Is a second osteotomy indicated? If so, is there a medical consensus on whether bone marrow implants promote osteogenesis? What about other implants of natural, artificial or combination materials? Are there any methods of reaming calcified bone for the purpose of pin insertion? Are there other remedies? Has anyone on the list seen varus deformities of the tibia recurring after an osteotomy? Would the Ilizarov device give better results within a reasonable time, taking into account age and impaired vascularity? And what other options exist that would straighten this thing out once and for all? I have copies of the June and October X-rays which can be sent as e-mail attachments off-list, and will be glad to answer questions insofar as possible.
Peter Miller
Date: Fri, 20 Oct 2000 12:15:23 -0400
From: J. Tracy Watson
An Ilizarov correction would certainly allow for gradual re-alignment of the deformity with a minimum of additional soft tissue disruption. If this is a hypertrophic nonunion then with distracton , these types of non-unions usually heal without additional bone grafting.. Time in frame is related to the extent of deformity and the quality of regenerate bone that forms in the distraction gap....
JTW
Date: Fri, 20 Oct 2000 11:04:58 -0500 (before xrays were available on this web page)
From: Adam Starr
Mr. Miller,
It's very difficult to make any comment without seeing your xrays, and the clinical condition of your leg. There are many ways to treat tibial malunion, and each has its pluses and minuses.
If there was no sign of infection, my vote would be to remove your plate, correct the malalignment, and place a statically locked intramedullary nail in the tibia.
The benefit of this would be that you wouldn't have to put up with an external fixator, we could correct the deformity right away, and it's likely you could start to bear some weight on the leg right after surgery. Reaming to create a channel for the nail to pass down your tibial canal would promote fracture union.
The risks of this technique are that, if there is any latent infection, the nail would spread the infection all the way up and down the tibia. Not an end-of-the-world disaster, but not a good thing to have happen. Also, the dissection required may lead to soft tissue loss, and the need for a flap.
You'll probably get a lot of differing opinions on this forum. There's not really an absolutely right answer. Hopefully you can get some info that will help you make an informed decision when you discuss this with your orthopaedic surgeon.
Good luck,
Adam Starr, Dallas, Texas
Date: Sat, 21 Oct 2000 08:21:55 +0900
From: Peter Miller
Adam Starr wrote:
> If there was no sign of infection, my vote would be to remove your plate, correct the malalignment, and place a statically locked intramedullary nail in the tibia.
That was the first choice of the surgeon who did the November 1999 osteotomy, but he found that the bone was totally impenetrable, it did not even bleed when cut. Such was (and presumably still is) the condition of the vascularity in that area, due to the damage from the 1971 trauma injury. Hence my question, Is there any way to place an intermedullary nail through that portion of the tibia that has become calcified or hardened? Or any other effective method of stabilization?
With best regards,
Peter Miller
Date: Sun, 22 Oct 2000 12:32:11 +0600
From: Alexander Chelnokov
THX for the x-rays. I already replied to the original message directly, without x-rays. After viewing can confirm that IMHO best option would be plate removal (leaving interfragmentary tissues untouched). And application of external fixatior with hinges. I would use 6 mm half-pins only not to transix muscles/tendons. After 2-3 weeks of stabilization as is, slow (less then standard 1 mm/day) distraction should be started. I would perform not only gradual alignment but over-lengthening 0.5 - 1 cm for a couple of weeks, then longitudinal compression.
Best regards,
Date: Sun, 22 Oct 2000 10:11:47 +0000
From: Bruce Meinhard
First I would evaluate the vascular status even going sofar as obtaining an angiogram. The next issue is would shortening but proper alignment be acceptable? If so, then one could perform a valgus osteotomy with lateral tension band plate or im rod as the canal could be drilled and reamed. If length were to be restored as well, then distraction over a rod or more classical corticotomy and correction of angulation and length could be achieved. The biggest risk os the limb vascularity but gradual distraction may be tolerated. The other consideration is the quality of the softtissues through which one must operate.
BPM
Date: Sat, 21 Oct 2000 11:58 PM
From: Bill Burman
>> Hopefully you will be able obtain some more valuable input regarding the management of this vexing problem. >>
>Yes, this will be quite useful. What I intend to do is try to select a >procedure, then a surgeon who is skilled and experienced in that procedure. My sense of the list is that the spirit of open dialogue is >ideal for revealing the nuances of the risks and benefits of each option.
Peter
High res images have been received and linked .
I haven't operated in over a decade so my opinion needs to be weighed accordingly.
If it were my leg I believe I would opt for the intramedullary nail treatment so that I could remain as fully functional as possible while waiting for my fracture to heal. Given the initial vascular injury and the signs of incomplete healing of the osteotomy after one year, that could be a long time. For the worst case scenario, intramedullary nail exchange (to prevent fatigue failure of the implant) would seem to be the least of all re-operation evils.
Xrays demonstrate that the medullary canal of the tibia has been obliterated in the vicinty of the fracture. It can be restored with sharp tipped intramedullary guide rods and end cutting reamers. This needs to be carefully done with fluoroscopic guidance.
If you can obtain a copy of Gerhard Kuntscher's book, Practice of Intramedullary Nailing, Springfield H, Charles C. Thomas 1967 from a medical library, a number of techniques are well described. One may involve osteotomies above and below an area of problematic healing to permit correction of translation and angulation.

A Photoshop mockup (without necessary plate removal) is included for your analysis. This of course is much easier to do on a computer than in vivo. Vascular and soft tissue concerns may prevent immediate full correction. That's where a case can be made for a preliminary, gradual and closely monitored deformity correction with external fixation.
A good digital photograph of the skin and soft tissues of the lower leg may better help decide this matter. I believe Bruce Meinhard's suggestion of preop angiography has merit. I wonder if it could be obtained less invasively with digital subtraction angiography. I can find no references for this.
As far as the downside of tibial intramedullary nailing I would recommend reviewing the OTA on-line debate between Charles Court-Brown and Augusto Sarmiento on this subject.
Date: Sun, 22 Oct 2000 09:02:19 -0500
From: Adam Starr
"Hence my question, Is there any way to place an intermedullary nail through that portion of the tibia that has become calcified or hardened?"
Yes. You can drill a hole through it and widen the hole using reamers. If the bone is completely avascular, I would cut back the bone until I reached some that bled. You really need living bone to get this to heal.
Then you could either 1) shorten the bone, to bring the bleeding ends together, and stabilize the construct with an external fixator (like a ring fixator, Ilizarov device); or 2) you could nail it out to correct length, leaving a gap where the dead bone used to be. You could fill that gap with bone graft, or a bone graft substitute.
I like nails more than I like external fixators. But there are plenty of surgeons who love Ilizarov fixators.
Good luck,
Adam Starr, Dallas, Texas
Date: Mon, 23 Oct 2000 02:06:33 +0600
From: Alexander Chelnokov
Hello Bruce,
Sunday, October 22, 2000, 4:11:47 PM, you wrote:
bman> First I would evaluate the vascular status even going bman> sofar as obtaining an angiogram.
The blood supply was at least enough to keep the foot alive, right? Even excellent main vessels doesn't mean good blood supply of the sclerotic midshaft area which looks definitely avascular or almost so, what played leading role in development of the situaton.
bman> The next issue is would shortening but proper alignment be bman> acceptable? If so, then one could perform a valgus osteotomy bman> with lateral tension band plate
The area already shows avascular changes. A plate at medial side has just been placed. Its replacement with lateral one hardly ever would increase local bone vascularization.
bman> or im rod as the canal could be drilled and reamed.
What bone defect is presumed if this would be done?
bman> If length were to be restored as well, then distraction bman> over a rod or more classical corticotomy and correction of bman> angulation and length could be achieved.
It would be a hard day for someone - plate removal, wedge resection, hard reaming and nailing, and application of external fixator with "miss a nail" wires/pins.
Maybe if closed nailing only without osteotomy performed, it could be a good shaft "endoprothesis". Tne patient would walk and bear weight. But still under risk of implant failure before union.
bman> The biggest risk os the limb vascularity but gradual bman> distraction may be tolerated.
Poor vascularity is more critical for open surgeries. Distraction usually increases blood supply, often dramatically - this is why it is used even in obliterating vascular diseases. Also often distraction decreases bone sclerosis - the sign means good prognosis for healing.
bman> The other consideration is the quality of the softtissues bman> through which one must operate.
One more argument for external fixation...
Best regards,
Date: Sun, 22 Oct 2000 15:24:24 -0500
From: Adam Starr
Hi Alex.
The main problem I have with external fixation is that it burns bridges.
Once those wires have been stuck through the bone, the medullary canal is colonized. So, if you ever decided to place an IM nail in the bone later, you'd have to accept a high, high risk of flaring up an infection, and spreading pus up and down the canal.
I recognize that many surgeons can achieve wonderful results with Ilizarov devices in the treatment of infected tibial non-unions. But, we get pretty good results here using IM nails, and, if the nails fail, we can always fall back to the ring fixator.
The reverse doesn't hold true. If you use a lizard rod, and want to convert to a nail for some reason (like maybe if the patient gets sick of having a ring fixator on his/her leg) you can't do it.
So, I think of ring fixators as a last resort. I know that there are lots of folks who feel differently, though.
As far as the difficulty of correcting the deformity, the worst thing I see in the films now is that doggone plate. The risk of occult colonization of that plate is about 30-40%, and it raises the specter of infection as the source of the current poor union.
I agree with you that a lateral plate is a bad idea. I think the medial plate was a bad idea.
The "hard day" correcting the deformity would be a hard day no matter what construct you chose. I don't think we would need to "miss a nail" with any ex-fix though. If I used a nail, I wouldn't need an ex-fix.
Adam Starr, Dallas, Texas
Date: Sun, 22 Oct 2000 21:34:26 +0100
From: nuno.lopes
We usually correct this kind of hypertrophic pseudarthrosis with axial deformity and shortening with a Ilizarov frame based on two hinges and a single motor.

The procedure to find the hinge point where one can simultaneously correct shortening and axial deformity is:
Date: Mon, 23 Oct 2000 03:45:43 +0600
From: Alexander Chelnokov
Hello Nuno
Monday, October 23, 2000, 2:34:26 AM, you wrote: mnp> shortening and axial deformity is: mnp> 1)- Draw the angle of deformity (a-c-b) finding the CORA - centre of mnp> rotation of angulation (c). If there are no shortening the correcting hinge
This mentioned sophisticated procedure is useful for corticotomy and one step correction with "guaranted" wedge-shape regenerate. In cases like this often angular correction only is not enough, and some cycles of distraction-compression (longitudinal and/or transverse) are needed.
And no big deal what first will be performed - lenghthening or alignment, so device can be assembled with four rods with hinges at their both ends to allow angulation as well as longitudinal traction-compression. Also distraction speed can be different - 1 mm/day at the center of bone for normal bone structure, 0.25-0.5 mm/day with days off stands for sclerotic bone.
Best regards,
Date: Mon, 23 Oct 2000 03:10:44 +0600
From: Alexander Chelnokov
Hello Adam,
Monday, October 23, 2000, 2:24:24 AM, you wrote: AS> canal is colonized.
But the colonization if any often shows no signs of infection.
AS> So, if you ever decided to place an IM nail in AS> the bone later, you'd have to accept a high, high risk of
Some literature exist about ex-fix with further replacement to nail in acute trauma. A new trend is lengthening over nail. So the factor is taken in account but doesn't prevent the approach. Though nobody forces us to change the modalaties - let them wear ex-fix as long as needed. Also "burning bridges" is maybe more suitable to internal fixation - once placed nail or plate, nothing you can change later, while you can play with external fixator at any moment to change position of bone ends and forces at the fracture site.
AS> Ilizarov devices in the treatment of infected tibial non-unions. AS> But, we get pretty good results here using IM nails, and, if AS> the nails fail, we can always fall back to the ring fixator.
How often this happens in infected tibial nonunions? I've seen many times how sclerotic bone ends behave in conditions of distraction. How do such non-unions with incongruent ends and sclerosis look like after closed nailing?
AS> The reverse doesn't hold true. If you use a lizard rod, and want AS> to convert to a nail for some reason (like maybe if the patient AS> gets sick of having a ring fixator on his/her leg) you can't do it.
To our experience, external fixation is more reliable way to reach union, though by expense of temporarily decreased quality of life. We here met patients with nonunions who were operated 5-10 times with different internal fixators and grafting - though without external frame, their quality of life didn't seem to be higher.
AS> So, I think of ring fixators as a last resort. I know that there AS> are lots of folks who feel differently, though.
This is IMHO mostly due to different regional preferences and fashions than to objective measures.
AS> occult colonization of that plate is about 30-40%, and it raises AS> the specter of infection as the source of the current poor union.
I am not sure that any infection is here at the moment, though i strongly agree that its high risk exists because of poor local blood supply. Bone sequestrae can later be infected from any endogenous source.
AS> The "hard day" correcting the deformity would be a hard day no AS> matter what construct you chose.
In case of ex-fix i don't think so. Plate removal, insertion of four half-pins, frame assembly and voila.
AS> I don't think we would need to "miss a nail" with any ex-fix AS> though. If I used a nail, I wouldn't need an ex-fix.
I agree that in this case a nail only looks better than the nail + a fixator for lengthening.
Best regards,
Date: Sun, 22 Oct 2000 16:50:45 -0500
From: Adam Starr
Hi Alex.
"Some literature exist about ex-fix with further replacement to nail in acute trauma."
These studies discuss early change from ex-fix to nails. Usually within a few days, or at most a couple weeks. The group at Shock Trauma recently published one regarding femoral nailing after provisional ex-fix for unstable patients (J Bone Joint Surg Am. 82(6):781-8, 2000 Jun.).
In their series, they exchanged the ex-fixes for nails at one week, on average. They had a few done at longer intervals - I think the longest was 50 days or so. They had about a 2% infection rate. The infection rate after closed nailing of closed fractures is less than 1%.
As far as I know, all these articles state that a history of infected pin tracts raises the risk of medullary infection if a nail is placed. It just makes sense - if the pins get pussed out, you have to assume that the bone is infected as well.
And, people who go into ring fixators are usually in them for a long, long time. Months and months and months. After such a long period of time, it's pretty much inevitable that the pins will be colonized. So, I would hesitate to put a nail in someone who'd been in a ring fixator for 6 months.
There was an article on lenghtening over a nail in JBJS recently (J Bone Joint Surg Am. 79(10):1464-80, 1997). It's a great technique for the right indication, but I'm not sure this patient needs to be lengthened, or needs to be in a ring fixator. I think we could correct his deformity, and stabilize his fracture, with a nail.
Also "burning bridges" is maybe more suitable to internal fixation - once placed nail or plate, nothing you can change later, while you can play with external fixator at any moment to change position of bone ends and forces at the fracture site.
If the nail fails, it's a simple matter to remove the nail and place an external fixator. You lose little or nothing, and the potential benefit is pretty great - healing and correction without the need for a ring fixator.
How often this happens in infected tibial nonunions? I've seen many times how sclerotic bone ends behave in conditions of distraction. How do such non-unions with incongruent ends and sclerosis look like after closed nailing?
It depends on what you did to the bone ends at the time of surgery. If the bone is truly dead and sclerotic, you could cut out the dead bone when you removed the plate. My preference would be to leave the gap this created open - I would ream to fill the gap with marrow, or pack it with bone graft.
To our experience, external fixation is more reliable way to reach union, though by expense of temporarily decreased quality of life. We here met patients with nonunions who were operated 5-10 times with different internal fixators and grafting - though without external frame, their quality of life didn't seem to be higher.
I agree that good results can be obtained with Ilizarov fixators.
This is IMHO mostly due to different regional preferences and fashions than to objective measures.
I agree with this, too. We like nails over here. Plenty of U.S. surgeons like ring fixators, too. I'm just not one of them.
Adam Starr, Dallas, Texas
Date: Mon, 23 Oct 2000 11:22:13 +0900
From: Peter Miller
> I'm not sure this patient needs to be lengthened,
The right tibia before osteotomy was 3 cm shorter than the left one. Most of this discrepancy was the result of the 22-degree varus deformity, not the 1971 injury. After the osteotomy and bone graft, the right tibia was one cm shorter, which I found acceptable. Now it is about 2 cm shorter (my estimate), which I do not find acceptable. Does the need for one or two cms of limb lengthening affect the IM v ex-fix choice?
Peter Miller
Date: Mon, 23 Oct 2000 10:29:56 -0400
From: E F Barrick
The method that I have found successful for reaming at least from the proximal end is to use an end cutting reamer that is attached to the shaft and then stiffen the construct by placing it over a smooth (not ball tipped) guide pin. To get across the distal side one would have to open the fracture site and bore it out with a Midex type device. Lots of bone graft. I would use an IM nail.
Date: Mon, 23 Oct 2000 19:54:49 +0600
From: Alexander Chelnokov
Hello Adam,
Monday, October 23, 2000, 3:50:45 AM, you wrote:
AS> within a few days, or at most a couple weeks. The group at Shock AS> Trauma recently published one regarding femoral nailing after AS> provisional ex-fix for unstable patients (J Bone Joint Surg Am.
Yes, i mean this article too.
AS> think the longest was 50 days or so. They had about a 2% infection AS> rate. The infection rate after closed nailing of closed fractures AS> is less than 1%.
Not too significant difference. AFAIR their series wasn't too large. But this article just demonstrates a possbility to change ex-fix to nail - their series was acute fractures, whicn had no local changes like this case.
AS> infected pin tracts raises the risk of medullary infection if a AS> nail is placed. It just makes sense - if the pins get pussed out,
Yes, definitely. So i would't insist that nailing has to be performed whatever happen.
AS> And, people who go into ring fixators are usually in them for a AS> long, long time. Months and months and months.
This happens.
AS> that the pins will be colonized. So, I would hesitate to put a AS> nail in someone who'd been in a ring fixator for 6 months.
If healing wasn't reached within this period in external fixatior I don't think that initial suggestion would be about to exchange the apparatus with a nail. At first we have to pay attention on what is going on around the gap and maybe do something else. If still decison is to replace ex-fix to a nail after 6 months or so, an external splint can be used after ex-fix removal until soft tissues are healed. The nailing can be scheduled within 4-6 weeks.
AS> to be lengthened, or needs to be in a ring fixator. I think we AS> could correct his deformity, and stabilize his fracture, with a nail.
The question as usual is how to calculate all risks properly.
AS> If the nail fails, it's a simple matter to remove the nail and AS> place an external fixator.
Is it always simple to extract distal part of the broken nail? I agree that closed nailing is very good option in general, but cases like this which are multiple operated, present shortening, has avascular changes, may require other treatment plan than just internal splint.
AS> You lose little or nothing, and the potential benefit is pretty AS> great - healing and correction without the need for a ring fixator.
"... the potential benefit is pretty great - healing and correction without the need for" a nail. :-) It sounds like ring fixator is itself a severe desease which we should avoid to reach great benefit.
AS> sclerosis look like after closed nailing? AS> It depends on what you did to the bone ends at the time of AS> surgery. If the bone is truly dead and sclerotic, you could cut
This may lead to unacceptable shortening. So what if only the plate would be removed and a nail inserted?
AS> be to leave the gap this created open - I would ream to fill the AS> gap with marrow, or pack it with bone graft.
I would love this plan looking at initial x-rays, before the osteotomy and plating. But what to do now?
AS> fashions than to objective measures. AS> I agree with this, too. We like nails over here. Plenty of U.S. AS> surgeons like ring fixators, too. I'm just not one of them.
Should we choose methods on the base of such emotional criteria? :-)
Best regards,
Date: Mon, 23 Oct 2000 18:26:25 +0200
From: Victor de Ridder
To all: we use the same method but have a smooth guide pin, without the usual ball, and have sharpened the end of the guide wire. This I can tap past the cutting reamer into the closed medulla to give the reamer even more stability. In our hands it has worked several times, even past the old fracture site/closed medulla into the distal shaft.
Greetings
Date: Wed, 25 Oct 2000 10:45:25 -0500
From: Steven Rabin
i've got to my email late and have seen all the discussion about rod vs external fixator and i think both are reasonable options when done by someone experienced in their use.
however, before deciding on method of fixation, i'd like to jump back to the beginning. The patient had a mild varus deformity initially which then progressed. Why did it progress? Is there a problem at the knee in addition to the tibial shaft deformity? I'd like to see better knee x-rays including standing mechanical axis views to be sure that there isn't a pre-surgery knee deformity complicating his later deformity.
in agreement with others, i think arteriogram would be very helpful. with the previous vascular injury, it would be useful to know where the arteries are and which are working even with good gross blood supply to the leg - in case it's infected and that sclerotic bone needs to be resected and he ends up with a muscle flap. It would also be useful to me to know where the vessels are if i went with the external fixator/ilizarov method. i'd hate to puncture an important vessel that happened to be in the wrong place due to previous deformity.
The ultimate success of the next surgery will as always depend on biomechanics. Correcting the alignment by whatever means should correct the mechanics, but No matter what technique is chosen, the bone won't heal if its dead. The failure of the plate fixation was probably because the osteotomy was done through very sclerotic avascular bone and the next surgery may also fail if the Biology part of biomechanics is not also addressed. I would strongly consider resection of avascular bone until live bone is obtained at both ends and then restore length and maintain alignment with the ilizarov method. Obviously, it might mean a long prolonged recovery period while length is achieved and the new regenerate bone is consolidates, but it would give the best chance of restoring the biology. If the patient strongly wants to avoid the ordeal, then IM rodding would help by opening up the canal, but i'd additionally add plenty of autologous bone graft, and possibly an implanted electrical stimulator in the hope that there is enough live bone to respond.
good luck.
Date: Thu, 26 Oct 2000 10:29:46 +0900
From: Peter Miller
In response to this request
> however, before deciding on method of fixation, i'd like to jump back to the > beginning. The patient had a mild varus deformity initially which then > progressed. Why did it progress? Is there a problem at the knee in addition to > the tibial shaft deformity? I'd like to see better knee x-rays including standing > mechanical axis views to be sure that there isn't a pre-surgery knee deformity > complicating his later deformity.

I am sending standing X-ray images of both knees for posting to the website. They show moderate osteoarthritis in the right knee and normal cartilage in the left knee. Knee pain was my initial complaint, and it was eventually diagnosed as resulting from the uneven pressure on the joint caused by the varus deformity. As to why the mild varus deformity of 1971 progressed to a 22-degree deformity in 1998, one answer I have received is that the 1971 fracture never healed properly.
Peter Miller, Kamakura, Japan
Date: Fri, 27 Oct 2000 00:27:14 EDT
From: Dave Sanders
Mr. Miller:
Interesting problem. Good luck with your decision. I personally favour h/w removal, resection of avascular bone, application of hinged transport frame, and gradual distraction/realignment due to fear of latent infection. If you could prove no infection was present I would lean the other way.
Adam, what is your plan if you open up the leg and find pus?
Best Regards,
Dave Sanders
Date: Mon, 30 Oct 2000 09:38:30 -0600
From: Adam Starr
"what is your plan if you open up the leg and find pus?"
If I found pus, I would use a ring fixator, I suppose. I would remove the plate, debride the bone and the wound, and maybe place antibiotic beads for a couple weeks. Then place a lizard rod.
If I didn't find pus, I would remove the plate, curette out the screw holes, and culture the plate. Then I would dissect the periosteum around the non-union site to expose the ends of the bone. I would find the medullary canal and open it. I would try to use hand reamers, but I would drill it if necessary. Then I would line the fragments up and pass a guide wire down the tibia. I would close as much of the periosteum as possible, close the wound, and ream it. I would do my best to keep the reamings in the wound. No tourniquet, ever.
I would measure his other tibia to get the right length.
Then I would nail it, and statically lock with 4 screws.
Then I'd let him toe-touch. And I'd wait for those cultures to come back. If they grew anything, I would suppress the infection with an appropriate antibiotic until the fracture healed.
Adam Starr, Dallas, Texas
Date: Mon, 30 Oct 2000 08:44:53 -0800
From: Chip Routt
adam-
i enjoy your lingo, it's folksy, makes me miss texans. sometimes i read the list and it feels like me and you are just sittin' roun' the campfire together...tellin' bone story, dadgummit.
but, for those list readers not "trying their durndest" to speak/type texan as their primary language, what exactly is a "lizard rod"?
is it like a "toady-frog's special purpose"?
or is it a component of a "magic screw"?
thanks from all us readers out here on the prairie.
happy trails-
chip
Date: Mon, 30 Oct 2000 12:08:09 -0500
From: J. Tracy Watson
Chip,
I thought I'd thoroughly discussed the derivation of "Lizard rod" with you....JTW
Date: Mon, 30 Oct 2000 12:18:59 -0600
From: Adam Starr
Chip,
No puede hablar? My apologies.
First time I ever heard anybody call them anything was when I was a 4th year med student on Charlie's service. I asked him what we would do with a nasty infected tibia non-union. He said, "put a lizard rod on it".
Dunno if I've ever actually heard him say "Ilizarov".
It wasn't until the actual operation that I saw "ilizarov" written on the instrument trays. My chief resident told me Ilizarov was a Russkie who operated wearing a chef's hat. Damned if it wasn't true.
Happy Halloween.
Adam
Date: Tue, 31 Oct 2000 18:29:45 +0500
From: Alexander Chelnokov
Hello Adam,
Monday, October 30, 2000, 8:38:30 PM, you wrote: AS> If I found pus, I would use a ring fixator, I suppose.
Monolateral frame can be used as well.
AS> I would remove the plate, debride the bone and the wound, and AS> maybe place antibiotic beads for a couple weeks. Then place a AS> lizard rod.
AFAIK stable fixation is crucial for treatment of infected cases so external fixator should be applied immediately if pus found.
Best regards,
Date: Fri, 16 Feb 2001 20:15:16 +0900
From: Peter Miller
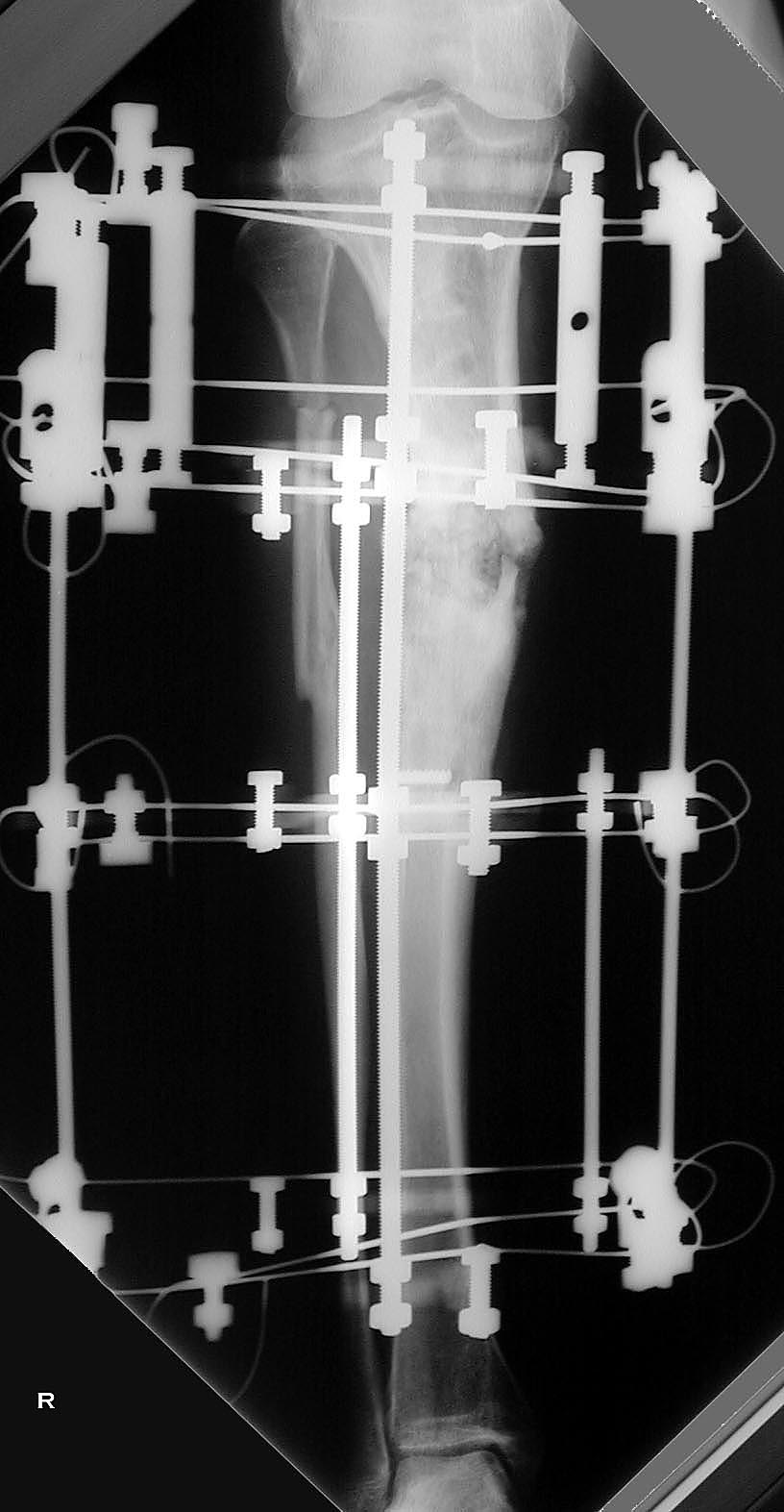
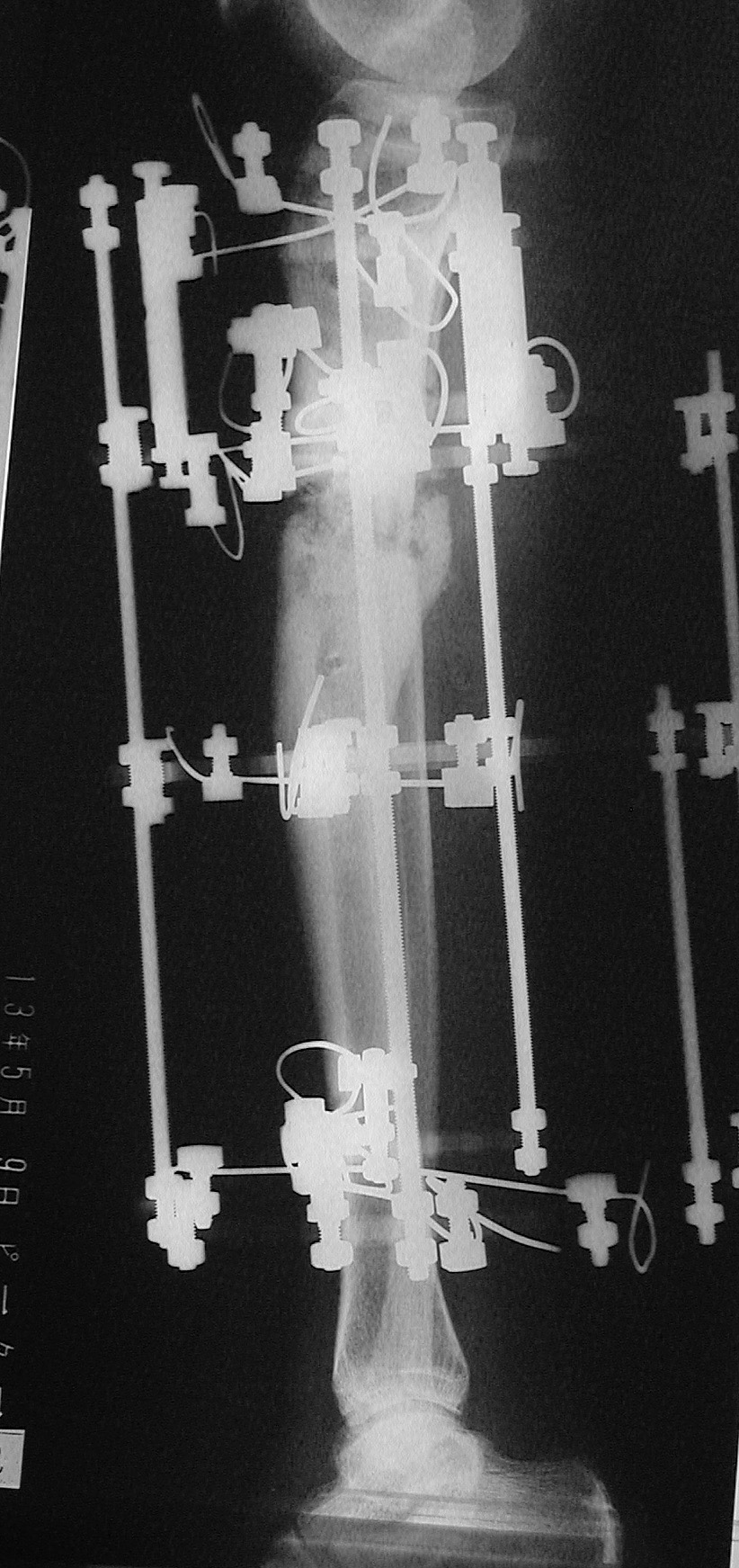
My 22-degree varus deformity of the tibia, the result of an earlier trauma injury, was corrected by Dr Tsuchiya and associates at Kanazawa University Hospital in Japan on February 7. Pre-op needle biopsy disclosed no infection around the fracture site. Bone scan tests with a radioisotope marker showed abundant blood flow around the fracture site. An Ilizarov frame mimicking the shape of the deformity was assembled based on the X-rays. All six screws of the former hardware, a titanium plate, were found to be loose. During surgery the tibia was found to be flexible enough to permit correction during the surgery. Bone graft material was harvested from the right iliac crest. A tissue culture of the plate from the previous, failed surgery revealed no infection. Antibiotic IV (Pansporin) was provided for five days, followed by oral Pansporin which continues. My temperature stabilized at normal within four or five days of the surgery, and there have been no signs of infection at the wire tracts. I started walking short distances three days after the surgery, and am currently undergoing physical therapy. The major limitations on my activity now are pain and stiffness, plus the usual post-op fatigue, but these are expected to diminish with time. The next step, of course, will be for regenerate to appear.
I wish to thank, again, the members of this group whose discussion of this case clarified the issues and helped me to select a treatment option. My selection of the Ilizarov technique was motivated primarily by the desire for a strong structural framework pending bone healing, and the documented boost in local blood supply stimulated by the Ilizarov device. The option I selected applies to the particulars of my own case, in which vascular damage and a previous failed surgery involving internal fixation figured prominently, and I do not attempt to draw any general conclusions from this one case.
 |
 |
 |
Pictures and X-rays are included. I will be glad to answer questions.
With gratitude,
Date: Fri, 16 Feb 2001 06:52:21 -0600
From: Adam Starr
Mr. Miller,
Thanks for the follow up info. It sounds like everything is going well.
Good luck in the future.
Date: Mon, 19 Feb 2001 19:49:23 -0000
From: Nuno Craveiro Lopes
Mr. Miller,
It seems you have resolved your problem!
Nevertheless, although a very stable external fixator, Ilizarov frame is not miraculous by itself! What makes the difference in what concerns the boost in local blood supply is not the frame but the regenerate of a lengthening procedure.
It is sure your leg will be fine with the cleaning and graft of the pseudarthrosis and static stabilisation with a Ilizarov frame, but this is not a Ilizarov technique, is a conventional treatment utilizing a Ilizarov frame as external fixator.
Best regards and good luck,
Date: Wed, 16 May 2001 22:23:25 +0900
From: Peter Miller
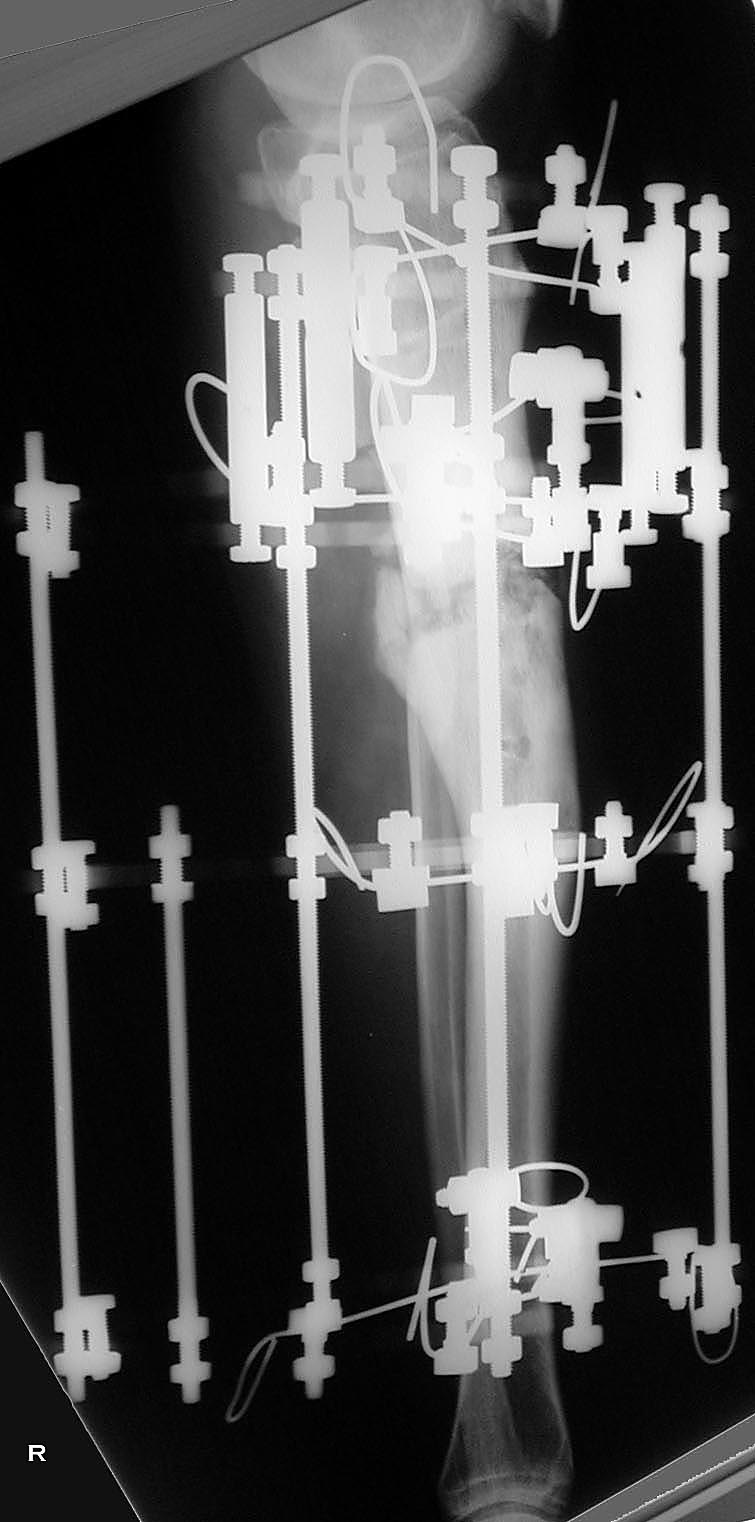
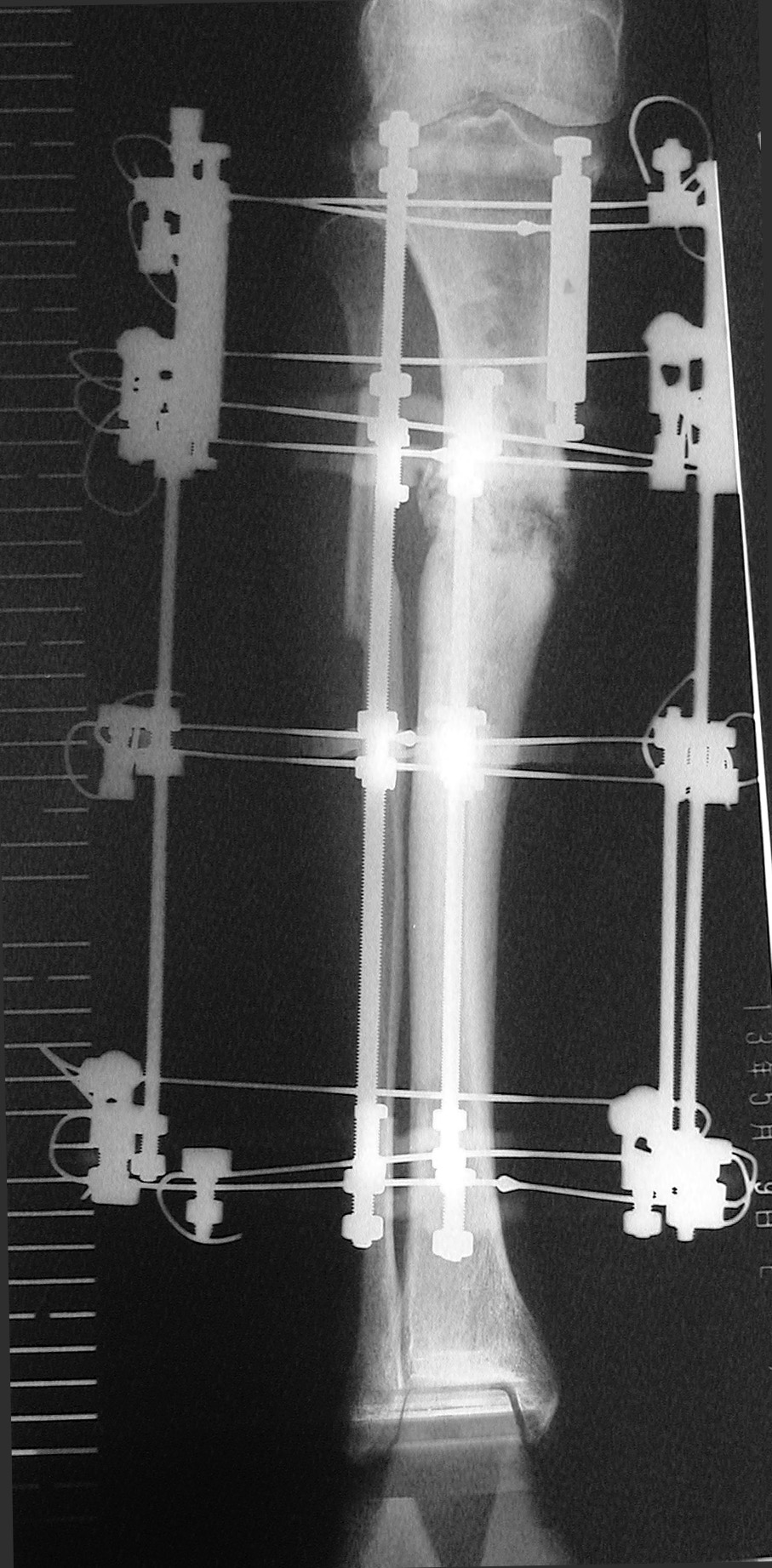
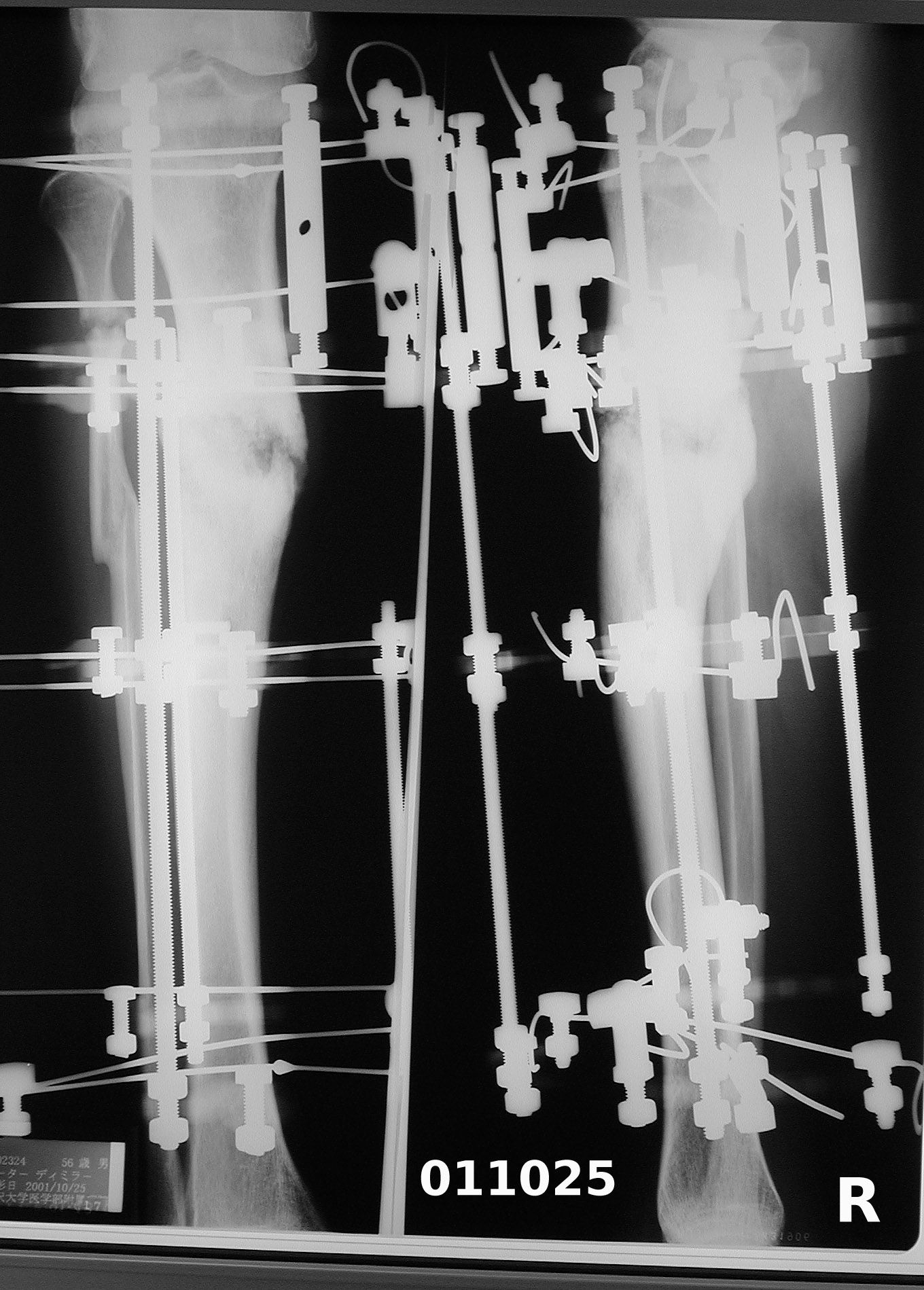
Attached are X-rays of my right leg three months after surgery with Ilizarov fixation.
 |
 |
According to the orthopaedic surgeon, they show solid callus formation on the medial side, while some gaps remain on the lateral side. There is no infection at the wire sites or anywhere else. The frame is to remain attached for one or two months longer. I find it to be much less of a burden than I expected. I am walking with full weight-bearing (no crutches or cane), though not yet with full balance, due to muscle atrophy. My walking is nearly pain-free, except for severe but transient pain in the center of the knee when descending stairs. I believe this is related to the unavoidably high placement of the uppermost wires, and it should cease after the frame is removed. As measured on the X-ray films, the difference in leg length is now five mm, compared with pre-op 3.5 cm. If the tibia continues to solidify and stays in its present configuration after removal of the frame, I will have escaped the judgment of Ecclesiastes 1:15 ('A crooked thing cannot be made straight'). I will inform the List of progress at six months post-op.
 |
The case just reported by Dr Kullerkann (varus deformity of upper tibia originating from trauma 20 years previously, and similar age) seems remarkably similar to mine. While I cannot offer a medical opinion on which method would be best for that case, perhaps my case can serve as useful data. One respondent mentioned ex-fix, and as a patient I can report that this method seems to be successful in my case. The length of time required in my case is related to vascular damage from the 1971 trauma. I am looking forward to my right tibia being in better shape than it has been for 30 years.
With best regards,
 |
 |
Also attached are pre-op and post-frame-removal pictures.
There was no infection during the entire 17 months of use of the Ilizarov frame, and only occasional minor skin irritation at a few of the wire sites.
Although the treatment took a long time, I am thoroughly satisfied with the outcome -- overjoyed, in fact. I will always be very grateful to the surgeons who did the work, to the people who maintain the OTA list, and to those list members whose vigorous debate informed my decision.
With best regards,
Peter Miller
Kamakura, Japan
Date: Wed, 04 Jan 2006 09:31:46 +0900
From: Peter Miller
Just a note to say that next month it will be five years since my Ilizarov surgery for severe varus deformity of the tibia. I don't have any X-rays to post because there's been no need to take any! But the results speak for themselves: I ski, cycle, trek, and walk everywhere.
I am enormously grateful to the surgeon in Kanazawa, Japan who did the work, to Dr Tracy Watson who recommended him, and for the vigorous discussion on Ortholist which led to the right decision.
Dealing with trauma as everyone does, I thought it would be good to know of a superbly successful and long-lasting outcome. I have had a big part of my life restored to me as a result of the difficult, risky, and exquisitely skillful surgery that was performed.
With best new year wishes,
Peter Miller
Kamakura, Japan