

Subject: Central Hip Fracture Dislocation
Referred to OTA List from: Indiaorth_list by Girish Kumar Fri, 31 May 2002 06:24:11 -0500
Date: Thursday, May 23, 2002 2:26 PM
Dear All,
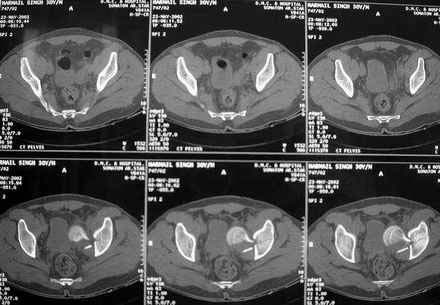
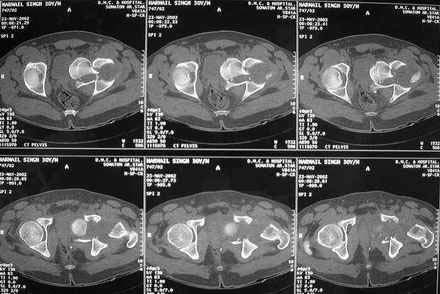
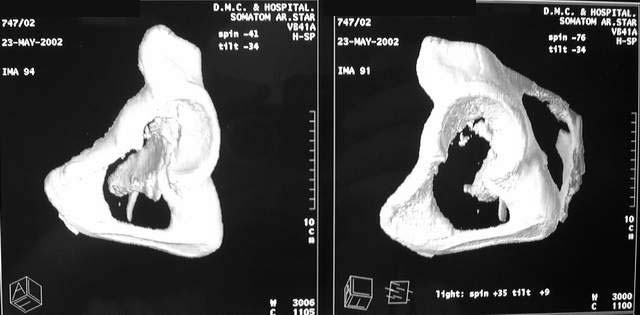
The Acetabular floor is also fractured as seen on CT scan images, I am attaching for your opinion.
|
|
|
|
|
Patient is ready for surgery and I have all kind of implants ready-----
Kindly advice what to do and how to proceed......approach, exposure , head extraction, how to build medial wall-----should it be like you did it with iliac crest cortical graft, or morcelised graft or should I try to get the fragment back from the pelvis.
I did not operate the case today as I felt I needed to be better prepared with implants and your advise.
Harpal
From: Mangal & Selhi
harpal,
this is not the kind of situation where one should do a total hip reconstruction IMHO. a thr is in essence a "cold", "reconstructive" procedure. using it as a reconstructive procedure for trauma is possibly stretching the indication a bit..... esp. when in the younger patient.
i would certainly operate to get the head out of the pelvis, reposition the fragments better to create as good a acetabulum for the future (maybe even morcellise the head, and leave it in the floor of what used to be the acetabulum), and treat him akin to a girdlestone for the present time.
i would be cautious, and wait for some consoldiation, maybe 9 months to a year, to have some semblance of an acetabulum, and then consider an uncemented prosthesis. that way he will possibly have a better long term outcome. this i think is one of the situations where good sense must prevail over technical ability and availibility
mangal
From: Girish Kumar
Dear Mangal & Selhi,
here is my opinion. please see if you agree. dr derek cooke from riyadh, saudi arabia did also contribute his opinion saying he would take the head out through the ilio-inguinal approach & bone graft the area in the same sitting & the do a 2nd stage uncemented rim-bearing THR 12 weeks later. that seems a good way to manage it, but I wonder whether a delayed THR would be enough in itself & avoid 2 procedures.
I agree with Mangal that this is certainly NOT the time to do a THR of any kind. Looking carefully at the CT And Xray images, the case is a central fracture-dislocation of the hip with a fracture neck of femur. the involvement of the antr and postr walls is not significant, mainly only the medial wall is involved. the femoral head is fully inruded into the pelvis. using traction is not going to bring the head out of this position. operating and removing this head fragment will be really difficult as there is no hold on this head to push & pull against.
I think IMHO that leaving it as it is and wait for the femoral head to resorb as will happen will be the best option so that there is no further trauma to this already seriously traumatised area and THR later will be a much easier option. if you think about it, the medial wall contributes very little to the stability of a THR anyway. the main areas of weight transmission are the superolat roof which seems intact here. there is an undisplaced fracture through the superior roof of the acetabulum which should heal fine with traction and bed rest, toe-touching WB thereafter.
This is only my humble opinion & what I would seriously consider in his best interests. even if the head did not resorb, which I doubt very much, it does not pose any problems in later THR. The ONLY need to take out this head fragment is if there is any ASSOCIATED urinary or other intra-pelvic compression due to this fragment. Remember also that there could well be bleeding by meddling and pulling out this piece which will be impossible to stop with our extra-pevic approach. I am thinking of cross-posting this case to the OTA lsit with Dr selhi's permssion,
Am sure it would elicit a lot of heated discussion......... Tough case and it will be even more tough to keep our itching surgeons hands off it now too....!!! let us know what you do and keep us updated.
With warm regards & best wishes,
Dr N V Girish Kumar
Date: Fri, 31 May 2002 10:47:39 -0400
From: James Carr
I had one exactly like this. It was diagnosed acutely, and I took it to the OR in the middle of the night. The femoral head pulled out easily- fortunately no pelvic vessel injury. I fixed the femoral neck, and he went on to bipolar hip at one year. I would do it now before things heal in and scar down. I would recommend pelvic angio. If the vessels look displaced/involved, it can be approached thru retroperitoneal approach as is done with medial migrated hip components (references exist in JBJS for this) The thought of leaving the head where it lies is interesting. You could then just do a hip replacement as per your preference. Take the head out later if needed. The acetabulum is split superiorly, and needs to be plated. On the case I had, the acetabulum spread nicely with a lamina spreader, and this helped retrieve the head. A standard cup has plenty of bone to support it because the ant/post/superior columns are present. However, failure to plate the acetabular fracture will likely result in the cup not fitting snugly, even with screws thru the cup (which I would recommend). I personally would give him a metal-metal hip.
Jim Carr
Date: Fri, 31 May 2002 08:20:53 -0700
From: Chip Routt Do you have patient information, injury history, physical exam, date of
injury, medical issues, etc.?
I wonder why it wasn't reduced and fixed urgently?
I've only seen this injury pattern in 4 patients, all young adults. They
were all referred late at night, or on a weekend. Three were/are
obese...maybe that's why they survive.
Each was treated with urgent femoral neck open reduction and stable internal
fixation, then the acetabular fracture was treated as its pattern dictated.
They have all healed. Two were without problems - one has nine years of
followup...she comes to the clinic annually as her "field trip" from the
jailhouse. The other has only one year of followup, so stay tuned.
The third patient developed a femoral neck nonunion with implant failure and
early focal aseptic necrosis, and was treated successfully with implant
retrieval and corrective proximal femoral osteotomy. He subsequently had a
hip replacement.
The fourth patient healed the fracture, but she has symptomatic hip pain
and aseptic necrosis. She is morbidly obese with a variety of confounding
issues.
Technically for your patient, the head/neck fragment is easily retrievable and
the quadrilateral surface fracture can be well reduced and stabilized using a Stoppa exposure and
intrapelvic plating. At the same anesthetic/prep/drape, the head/neck femoral
fracture can be reduced and stabilized using an anterior exposure of the hip
joint...I'd use a Smith-Petersen interval. The neck fracture fixation screws are
inserted percutaneously in this situation after the open reduction is clamped.
Chip
M.L. Chip Routt, Jr.,M.D.
Date: Fri, 31 May 2002 10:47:29 -0500
From: Adam Starr
This is a bad problem for this 30 year old guy. I wonder what "can afford" means?
I've had one like this. My patient was a 50 year old lady. Her acetabular
fracture was worse. We fixed her tab fx the day she came in, and anatomically
reduced the femoral neck fracture. The ligamentum teres was still attached to the
head. Her tab healed well, but the head went on to AVN at one year. She underwent
a total hip replacement and has done well.
In this patient, it's too bad he's 2 weeks out.
You'll need to be able to get to the quad plate to reduce and fix it. Maybe a
stoppa approach.
If, by some miracle, there is some soft tissue still attached to the neck, you
could try to stuff it back through that hole. It probably won't fit. It looks
like the tab opened up wide to let the head into the pelvis, then slammed back
shut and trapped it. I bet that crack in the dome was displaced a lot when the
injury occurred.
So, you'll probably have to take the head fragment out through your stoppa approach.
Once you've got the quad plate piece reduced and fixed, I would fix the
fracture at the dome with screws placed from the AIIS to the PIIS.
Far as the neck fx goes, I vote for anatomic reduction and fixation. I would
use a smith-pete approach. You could use cannulated screws, or even standard 6.5
screws to hold your reduction.
Adam Starr
Date: Fri, 31 May 2002 16:07:13 +0000
From: b.meinhard
Although a case report does not a series make...I published such a case in the
JBJS American (J Bone Joint Surg Am 1987 Apr;69(4):612-5), where I removed the
head through the hip capsule and fixed it with cannulated screws. I then
performed a primary muscle pedicle
bone graft to the femoral neck as described by
Meyers. The patient did well . If there is medial instability, one can add an
ilioinguinal approach to graft and or place spring plates for medial support. I
would prefer this to performing a total hip replacement in such a young person.
B. Meinhard, MD
Date: Mon, 3 Jun 2002 23:50:33 -0500
From: girish kumar
Jim Carr: I had one exactly like this . . . I personally would give him a metal-metal hip.
this case is 2 weeks old, has had a popular treatment round these parts,
still so unfortunately, of native oil massage which causes a lot of
fibrosis and heterotopic ossification. this same oil massage done around
the elbow results in massive volkmann's contractures too, as you might have
read in books. we actually see it here clinically even today, very much
less in my part of south India than up in the north.
back to thic case, I am recommending delayed THR so the fracture would have
healed well by then. the laminar spreader use in this case is very
interesting indeed.
what metal-metal hip are you using? how long have you been doing it? do you
trauma guys do elective THR's and TKR's as well?
Dr N V Girish Kumar Date: Mon, 3 Jun 2002 23:50:32 -0500
From: girish kumar
hi, answering chip routt's and adam starr's questions and queries in one go.
thanks for your input. agree with most of it.
>Do you have patient information, injury history, physical exam, date of
injury, medical issues, etc.? I wonder why it wasn't reduced and fixed urgently?
young fit 30 yrs old patient, presents 2 weeks later after oil massage native
treatment no other injuries, sciatic palsy etc. no AV injury clinically. no
dopplers done to confirm this though. can't tell you exact mechanism of injury,
will ask and let you know.
>Technically for your patient, the head/neck fragment is easily retrievable
and the quadrilateral surface fracture can be well reduced and stabilized
using a Stoppa exposure and intrapelvic plating. At the same
anesthetic/prep/drape, the head/neck femoral fracture can be reduced and
stabilized using an anterior exposure of the hip joint...I'd use a
Smith-Petersen interval. The neck fracture fixation screws are inserted
percutaneously in this situation after the open reduction is clamped.
yes agreed, an ilio-inguinal or stoppa approach will be necessary to get
the head out. also grafting can be done simultaneously. but question is -
will this be highly necessary if we are planning an elective THR in 3 mths
time after the dome split fracture has healed fully with conservative
management. here in india, most patients are not insured, want 1 surgery to
do everything and are highly unrealistic in their expectations. that is
just one point to be remembered in suggesting a course of treatment, but
not to be allowed to decide the whole course of rx. so the term "can
afford" is all important, in deciding whether we need to rack our brains to
decide on what surgery we can do! if he cannot pay for treatment, it is
only an academic excercise to improve our management plans and protocols.
my point is, leaving the head alone as it is 2 wks old fracture, has been
massaged and moved, unitl presenting to the tertiary centre, is better than
"heroics" of fixing it now. am sure there is no reference on delayed
internal fixation for this type of fracture, with the severity of injury
which must have caused it. so with fixing the head out of the equation, is
there any advantage in fixing the quad plate and grafting?? granted that as
much bony contact is better in an uncemented cup for long term success, can
we not just do cancellous bone grafting of the medial wall in delayed
setting at the time of elective THR in 3 mths time?? this would be better
than staged surgery as all the advantages of grafting, THR are all there
without the added surgical trauma of plating, another exposure, cost etc.
what do the you all think about this approach?
With warm regards & best wishes,
Dr N V Girish Kumar Date: Tue, 04 Jun 2002 10:47:08 -0400
From: James Carr
Primary THR in young man like this is certainly controversial. I mentioned
metal on metal, but metal debris is a concern. I have been doing them since
release a few years back, but certainly it does not have the f/u like other
systems. Delayed approach is just fine.
Jim Carr
Date: Tues, 4 Jun 2002 11:30 AM
From: Bill Burman
>if he cannot pay for treatment, it is
only an academic excercise to improve our management plans and protocols.
Dr. Kumar Thank you for contributing this case. Given the economic constraints
described in your posts, I am wondering if even delayed THRA is advisable
for a 30 year old active male. According to the literature, the likelihood
of a necessity for revision surgery in such a young patient would be high.
According to Maloney, JBJS 83A:1582 2001, THRA revision burden in the US
is 18% of 200,000 total hips done in this country per year. The average
cost per revision is $19,200. The total cost is $691 million/annum - a figure
that is (for a smaller population with a relatively robust economy) increasingly
difficult to afford. Given the reports of apparently tolerable results with procedures
such as girdlestone which occassionally appear from your part of the
world , I am wondering if you can tell us whether these are indeed viable
options or are such reports in some way flawed? Date: Wed, 5 Jun 2002 00:13:30 +0530
From: DR T I GEORGE
Hi Bill,
In our institution we still manage to convince younger patients about
arthrodesis of the hip as a good option and many do accept it. I wonder what
is the experience with others.
DR T I GEORGE,
Date: Wed, 5 Jun 2002 23:01:29 -0500
From: girish kumar
dr burman,
thanks for your interesting response. yes, you are quite right in
suggesting the option of girdlestone hemiarthroplasty in certain
"economically constrained" situations. i am sure this pertains just as much
to the US as it does in India in certain economic groups. Am I right in
saying this - in Medicare population etc??? DO confirm this point for my
knowledge of medical needs around the world.
also, with reg. to this particular case, the line which said - " can
afford" is all important. BUT whether he can afford a second & third &
..... much more expensive revision with not so acceptable results as well
is another matter.
we "overseas" trained surgeons are not at all familiar with Prof Tuli's treatment & results of this technique. if it does
work as well as he has suggested, it may be more ideal than the present THR's as
our patients(rural & lower socio-economic group) like to and do squat crosslegged
on the floor routinely incl. the "Indian" toilet which requires squatting with
feet flat on the ground & abdomen-thigh-calf in Z apposition(wow, hope somebody
understands what I mean!!!), as in the picture in prof tuli's paper on the hwbf
website. however, even locally, there is a dearth of research & cases to look
into this difficult problem. but also remember that I can do a THR here for at a
rock-bottom charge of Rs 80,000 to 100,000( or USD 1750 or 2200...!!!) including
the cost of imported Charnley Elite or some such standard imported prosthesis at
rs 40,000 or so. even a TKR, I can do at slightly higher prices, but nowhere near
the costs reached in the USA or in the West. Also remember that I have only
imported equipment like a Synthes drill , Smith & Nephew & Arthrex arthroscopy
stuff etc as you would have there. But it is a sad fact that even at this cost, a
lot of our population are unable to afford it. Of course, if you send me a
patient from the USA, I would like to charge a bit higher to enable me to buy
another new piece of equipment or have the luxury of a holiday ;-))
Dr N V Girish Kumar Date: Thu, 6 Jun 2002 06:32:01 +0100
From: rajesh
I hope Dr.Girish Kumar does not mean to generalise when he says " overseas
trained doctors". Before becoming overseas trained, most of us are actually
trained in India and are aware of Prof Tuli and his
girdlestone followed by several weeks of skeletal traction. (at least, we
should be-there is no point in forgetting ones roots, I think - a good method of
treatment is a good one whether it is developed in India or elsewhere). He has
written a very good monograph on Treatment of tuberculosis of joints as well.
I don't think one can actually compare prices and say a THR done with
"imported" implants is cheaper in India - the purchasing power of ?1 or $1
is not really the same as 1 Indian rupee! Are people without medical
insurance treated very badly in the US? In the UK the National Health
sevcice, for all its faults, does deliver free health care at quite a good
quality most of the time and it is indeed a relief not to have to think
whether a particular patient can afford to get the best treatment.
And as someone said, it does not really hurt to advertise a bit as well ;-)
Mr.K.Rajesh, MS(Orth), DipNB(Orth),FRCS,FRCS(Orth)
Date: Thu, 06 Jun 2002 09:43:36 -0500
From: Adam Starr
Dr Kumar,
I'd never pretend that delivery of surgical trauma care in the USA is perfect,
but I can tell you that a patient with an acetabular fracture who arrives at our
hospital here in Dallas will be treated regardless of his/her ability to pay.
We don't make surgical decisions based on insurance status or Medicare status or
whatever. The hospital I work at is a county hospital that receives county, state
and federal tax money to support its care of indigent patients.
If we didn't get that tax money support, the hospital couldn't run.
The hospital WILL bill the patient for services provided, and if the patient is
truly indigent, we'll try to enroll them in a "managed care" program for indigent
patients.
Adam Starr
Date: Thu, 06 Jun 2002 14:56:39 +0000
From: b.meinhard
I can echo what Dr Starr had to say , and add that since
my public hospital is in the east coast near Kennedy and
Laguardia airports, we often receive alien patients
sent by their families with severe medical
conditions..including patients from India,for whom we
are required to treat with the highest standard of care
in the community ,REGARDLESS OF THEIR ABILITY TO PAY.
Again not perfect, but we take the good with the bad.
BPM
Date: Thu, 6 Jun 2002 11:59 AM
From: Bill Burman
Drs. George, Kumar and Rajesh
Thank you for your interesting replies.
"economically constrained" situations. i am sure this pertains just as much
to the US as it does in India in certain economic groups. Am I right in
saying this - in Medicare population etc???
This is true. Medicare is the main health insurance provider for patients over
65 in the US. With the sharply rising cost of medical care, the Medicare trust
fund faces serious depletion. As noted in the CATC Reports circulated by Jeff
Anglen to this list, the US Congress faces hard choices and is debating whether
to cut payments to doctors or prescriptions to seniors. Some doctors here
now say they will have to stop taking care of Medicare patients.
Are people without medical
insurance treated very badly in the US? In the UK the National Health
service ,for all its faults, does deliver free health care at quite a good
quality most of the time and it is indeed a relief not to have to think
whether a particular patient can afford to get the best treatment
We have a complex healthcare system in the US. One has to have an MBA and go to
years of business school to understand it. It is one which will not routinely
provide for health maintenance (e.g. hypertension meds which a senior citizen on
a fixed income may not be able to afford). However, should that patient blow-out
a cerebral vessel, the price of treating a persistent vegetative state with 2-3
weeks of intensive care is generally paid (in part for fear of contingency fee
litigation) through cost shifting to those with insurance or a higher tax burden
to cover the public hospital's bad debt. The price of that medical care probably could
have bought hypertension meds for a whole city that year.
Speaking personally, I am very proud of the sort of medical
care that colleagues such as Drs. Starr, Meinhard and others in our public
hospital system provide (even though there is a resemblance of it to a National
Health Service).
Date: Thu, 6 Jun 2002 22:51:10 -0500
From: girish kumar
hi all,
"interesting" how discussions on the OTA list always turn out into
"controversies"!!!!! which is why I like this list so much for its vibrancy
& deep sense of righteousness and integrity. i hope it keeps it up for ever
& ever - will remain rooted to the list for as long as that is so.
I have learnt a lot from this thread reg. the way the US system works
though I am yet to get an MBA ;-)
whatever my e-list colleague dr rajesh says, i would like to add the
following points reg the healthcare system in india.
the private sector is totally cut off from state funding and hence cannot
afford to treat non-paying patients routinely. there is a move to have some
funding channeled for some specialities and some cases, but overall it is
not enough. trauma is certainly not an area where this is so now, like it
or not. this is sad, bad and mean, but that's the way it is & it doesn't
help to brush it under the carpet. i like to state things - warts and all,
hoping to improve things. but let someone come out and say i am wrong in my
facts.
the state system is entirely separate & by God, I would not want to be
admitted and treated there in my state anyway. there are centres which are
quite good, but overall it is not impressive frankly speaking. we can only
improve when we admit there is a deficiency.
yes, i "love" the NHS(as it used to be, i must add ;-) ) and its
egalitarian ethos and service to all, but i do not think it is so now from
what i hear.
prof tuli is a great man, but i must say i have never any case treated in
such a way in my 2 yrs in ortho training in madras before going to the ~UK
and would love to hear from colleagues who are familiar with this method
and enlighten me and others on this list as to how good it is in real life
& practice. if it is as good as it seems, why do a THR at all? obviously it
is not as good, for other wise we would be doing more such excision
arthroplasties routinely.
And as someone said, it does not really hurt to advertise a bit as well ;-)
why not, especially if it is true......;-))
come on rajesh, we should rise above "national" and other limits and speak
the truth even if it hurts. i came back to india voluntarily as i am
patriotic and deeply "indian". but let us not hide from the truth. i am
sure we all agree there are a lot of improvements necessary in the state(ie
Govt)medical system.
rajesh, so please tell us your personal experience of excision
arthroplasties similar to prof tuli's article and how good they were in
your opinion.
thanks to all for the wonderful replies.
Dr N V Girish Kumar Date: Fri, 7 Jun 2002 06:22:05 +0100
From: rajesh
I am sorry if I have been the cause for turning this list into a less
academic one with my comments.;-)
Couple of things- I have NO experience of excision arthroplasty,never said I
did. Reason why we don't do it more often ? -not needed in the UK for the
majority of cases as the NHS absorbs the cost.I have tried to interest some
consultants I worked with to try to use it when infected THR's are removed
but nobody was really keen to try a 3rd world method which even the 3rd
world surgeons were reluctant to use.( not sexy enough like a THR? can't
charge as much as a THR? "if the doctor down the road can do THR why do you
want to do an excision?" )
Why the situation does not change in India ? - too many "patriotic " people
keen to accept that things "cannnto change" and not enough people trying to
change things.(not really worth their while,is it? when patients are willing
to pay for their operation,who cares about the ones who cannot-send them to
the government hospitals !)I know two of my friends who went back to India
from the UK who have made arrangements with their hospital to allow them to
operate on poor patients with massively reduced charges, no surgeon's fee
etc.It is not difficult to do but obviuosly not going to make much of a
difference in the large scale of things.Also as one of them said,his
colleagues are quite happy to let him do this because that means atleast
some of the paying patients will filter down to them because he is too busy
with the poor !
If people actually tried to make the government hospitals better instaed of
saying"I would not have myself treated there" things could improve but it
has been going on for too long and as long as politicians know that they
will not suffer (best private hospitals, best surgeons etc available to
them) it will remain like that.Sad but true.
If I were going to offer to operate at reduced rates on people from the
states or UK or wherever,I would make sure that each patient contributes
toward buying some implants in order to benefit the population(maybe sponsor
a THR if they were having one done?)We used to make patients who could
afford buy 2 sets of implants when we were doing our training in India (2
nails instead of one etc - as patients had to buy implants in our medical
college)so that we had a common pool of spare plates, screws, nails etc when
we needed them for a poor patient.We also managed to get the medical reps to
donate screws etc from their company.Is it that difficult to do that? I
recently met some of my colleagues who are assistant professors and
lecturers in my previous medical college and apparently they are still doing
that for trauma implants eventhough nobody is really keen (or rich enough)
to buy two sets of hip replacements,it seems ;-)
Once again, sorry for straying from the academic.
rajesh
Mr.K.Rajesh, MS(Orth), DipNB(Orth),FRCS,FRCS(Orth)
Date: Fri, 7 Jun 2002 15:31:43 +0530
From: DR T I GEORGE
Dear Girish Kumar and Rajesh,
It is a litle saddening that we have downgraded our discussion forum to a
non -Orthopaedic platform. If all of us are interested in improving the
system in India I feel we should discuss this in Indiaorth discussion group
where we will get more constructive and practical contributions from people
who have been in India for years and have first hand experience. We all know
that you both take part in Indiaorth discussions. Let us not wash dirty
linen in public.
SORRY IF I HAVE HURT YOUR FEELINGS.
DR T I GEORGE,
Date: Fri, 7 Jun 2002 18:14:05 +0300
From: Alo Kullerkann
Dear Members,
I would like to say a word for so called non-academic mailings.
Why not to discuss things not straight related to fracture, surgery technic,
implant or etc.? I read with a great interest of mailings from Drs Rajesh and
Kumar. Not that I favour "need one, need to buy two" but its just interesting how
orthopaedic related things keep going around the world. Orthopaedics is an art
that has many facets and one of them is a management. I wouldnt say that we
should start deep discussion about one or another narrow topic, but implant
feeding is certanly one part of it, even in developed countries where one can
afford the best treatment for the patient not having to think how much it costs.
Last but not least - there is always a delete button on your screen :-)
Best regards,
Alo Kullerkann, MD.
Date: Tue, 11 Jun 2002 11:01:24 -0500
From: girish kumar
Hi Rajesh,
points well taken indeed.
lots of good points, wil mull over and see what i can do to immprove the
situation. i am having a full range of imported instruments and expertise
to provide care at "subsidised" rates. one thing i can vouch for is high
quality care if they come to me. but yes, as a part of society, there are
things that need to be done to improve the working of govt/state hospitals
too, as a large sector of poulation cannot afford the private care
facilities. i am having a full range of imported instruments and expertise
to provide care at "subsidised" rates.
Talked to a surgeon from Salem, a smaller city where I visit once a month
for arthroscopic & arthritis surgery, he mentioned seeing a few cases and
having done an excision arthroplasty for an infected hemi-arthroplasty,
with reasonably good results. I will try and track him down and get some
pictures for the list. He says the there will be a limp, but the patient
will be able to walk around the office etc, but may not be able to do a
labouring job, which is ruled out anyway after a THR(!!). It seems a
worthwhile option if circumstances dictate, just that it will take some
time to settle down to a reasonable activity state what with intial
traction and then prolonged limited mobilisation status. have to thank bill
burman for bringing this article to my notice, my colleague from salem also
denied knowledge of this particular publication by prof tuli. so it is very
interesting to see how convoluted the route of knowledge has been here &
again brought into focus the educational aspect of such email lists.
indeed, india is going to turn into a healthcare exporter soon, with
lower-cost hitech surgery, the only thing needed is tightening up protocols
to enable really high quality consistently all the time. so i will only be
too glad to offer my services at a "reasonable" cost to those willing to
come over. charges are not what our profession is about - primarily, i
mean.
as allo said, it is not only technical expertise that makes a successful
surgeon, esp. in the private sector ;-)
Dr N V Girish Kumar
Professor-Orthopedic Surgery
Harborview Medical Center
Seattle, WA
Dallas, Texas
Consultant Orthopaedic surgeon,
Polytrauma, Microvascular Surgery and Hand Surgery Unit,
Metropolitan Hospital, Trichur, South India.
Locum Consultant
Tameside General Hospital
UK.
Dallas, Texas
Locum Consultant
Tameside General Hospital
UK.
Consultant Orthopaedic surgeon,
Polytrauma, Microvascular Surgery and Hand Surgery Unit,
Metropolitan Hospital, Trichur, South India.
Orthopaedic Resident
Mustame Hospital, Tallinn
Estonia
{kind=link}