


Date: Thu, 9 Jan 2003 01:03:40 +0500
Subject: Sequelae of tibia/ankle injury
Hello All,
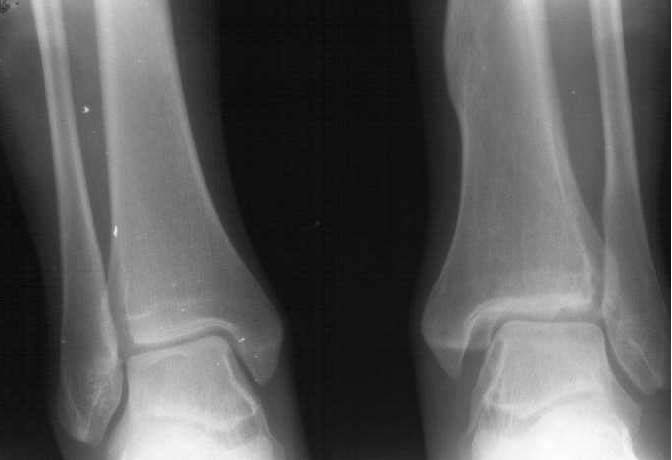
A female 14 y.o. sustained a spiral fracture of the distal tibia 1.5 years ago (Image 1). She was treated elsewhere by closed retrograde nailing with a thin nail (Image 2). The nail was removed after healing.
Comparative images of both ankles AP (Image 3) and Lateral view (Image 4) - in standing with loading are provided.
Now her complaints are pain and swelling around the ankle after loading and mediolateral instability because of deficiency of deltoid ligament and syndesmosis. No pain at rest. Ankle ROM is almost full.
It appears at the postop films that a small fragment was impacted to the joint medially, and displacement of Volkmann's triangle was increased a bit. Now we see early appearance of ankle arthritis. What should be done with the patient? It looks too early to fuse the joint. Ankle revision, modelling resection/arthroplasty? Ligament repair? Something else?
|
|
|
|
THX in advance.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Thu, 9 Jan 2003 06:30 AM EST
From: Bill Burman
Alex
Jarvis and Firoz in J Trauma 2001;51:714 report the association of an external rotation triplane fracture (typically seen as Salter-Harris III in the AP and Salter-Harris II in the lateral) with distal spiral tibial fractures.
It is difficult to tell from the post retrograde im nail images but there is definitely an SH II on the lateral and possibly a SH III (tillaux fragment) in the region of the tubercle of Chaput.
The retrograde IM device may have maintained a > 2mm displacement of the triplane fx which according to Ertl et al JBJS A 70: 967 1988 generally gives a poor long term outcome. Do you have access to injury films and what about bilateral comparative axial CT's to better define the ankle mortise pathoanatomy?
Date: Thu, 9 Jan 2003 07:25:00 -0500
From: James Carr
Alex
I would obtain a CAT scan.
Jim Carr
James B. Carr, MD
Palmetto Health Orthopedics
Date: Fri, 10 Jan 2003
Hello Bill,
generally gives a poor long term outcome. Do you have access to injury films
Preoperative x-ray was attached to my initial posting.
and what about bilateral comparative axial CT's to better define the ankle mortise pathoanatomy?
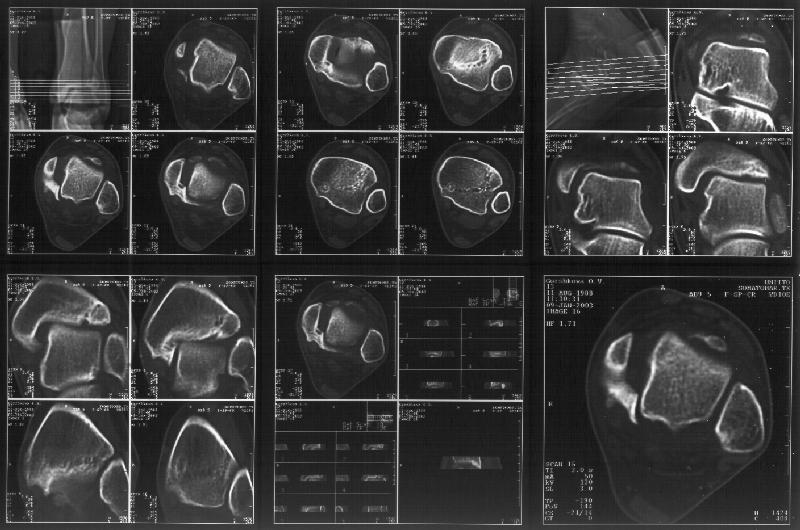
I attach CT of the affected ankle.
 |
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Fri, 10 Jan 2003 09:17:26 -0600
From: John Early
Interesting case. thanks for the ct cuts. now it is real clear that there is a posterior medial maleolar fragment displaced into the joint forcing the talus laterally. My first inclination in this young girl is to debride out the displaced fragment. The difficult part will be visualization ot know how much to take. My approach would be through an oblique medial malleolar osteotomy and hinge the distal malleolus away from the talus leaving the deep deltoid intact. this way you could easily view the whole articular surface of the medial gutter. I would debride the prominent bone back slightly beyond the level of the normal malleolar surface. The osteotomy may also help reduce the widened mortise. I don't see anything i would do to the syndesmosis area nor any significant length differences between the fibula and tibia laterally form the proximal tibia fracture.
John Early MD
U Texas Southwestern Med Ctr
Dallas, Texas
Reference: Alexander, I.J. and Watson, J.T.: Step-Cut Osteotomy of the Medial Malleolus for Exposure of the Medial Ankle Joint Space. Foot and Ankle, pp. 242-243,February 1991
Date: Sat, 11 Jan 2003 10:30 EST
From: Bill Burman
Alex
The CT seems to show residual triplane fx lines.
I wonder if this could have been a 4 part triplane with an intra-medial malleolar component as described by Von Laer JBJSA 67:687 1985 which was displaced by the im device?
John Early's suggestion of posterior medial malleolar debridement and possible medial malleolar repositioning for mortice narrowing is very interesting. You mention that the patient already has mediolateral instability. While it does push the talus laterally, it looks like the posterior medial malleolar fragment may be providing a congruent buttress against medial talar displacement. If that were removed and the mortise was not in some way narrowed - the mediolateral instability might increase.
I wonder if comparison CT cuts of the normal ankle and possibly 3D reconstruction/modeling might give a better understanding of the pathoanatomy.
Date: Wed, 15 Jan 2003 20:56:30 +0500
From: Alexander Chelnokov
Hello Bill,
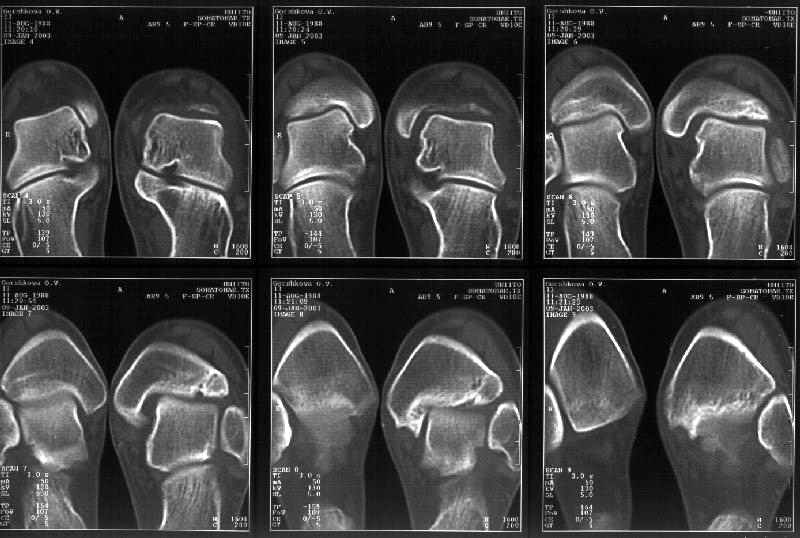
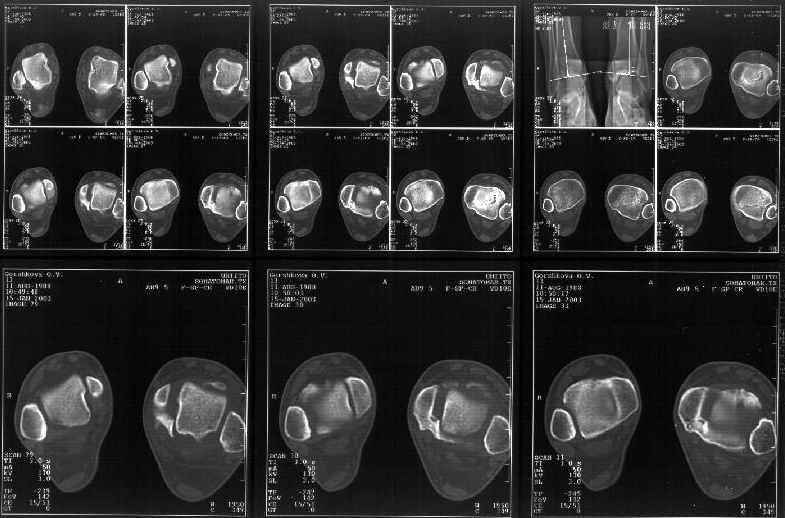
Today the axial and frontal cuts were performed - attached.
 |
 |
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Wed, 15 Jan 2003 17:07 EST
From: Bill Burman
Alex
The injury films show an external torsional fx of the distal tibia - the typical triplane fx mechanism.
External rotatory displacement of the tillaux component would act to widen the mortise.
The comparison coronal and axial CT show a tillaux component and a widened mortise which was probably first held open by the im device and then the malunion of posterior medial malleolar fragment - drawn into the joint by the deep deltoid talar attachment.
With posterior medial malleolar fx excision alone, mediolateral instability could increase. The wide mortise, a result of multiplanar fx deformity, needs to be narrowed - but how can this be reliably achieved? Perhaps a 3D model is needed ala
to help decide what correction, if any, can be applied. I get no hits on a Medline Search for "triplane" and "malunion".
Date: Thu, 16 Jan 2003 09:21:06 -0500
From: James Carr
Thanks for the CT. Did she have a higher fibula fracture? I believe she has an external rotation malunion of the posterior malleolus/lateral plafond/ ?fibula. The entire segment displaced laterally and rotationally in relation to the medial malleolus, which stayed home. The talocrual angle is approx the same on each ankle, so I agree the fibula is out to length. I would arthroscope the ankle to visualize the articular surfaces.
I think recreation of the original fx lines and repositioning would be ideal, but most difficult. I would try to osteotomize the medial malleolus in a coronal plane just in front of the malunited posterior piece, and in the usual saggital plane at the rounded "shoulder" of the malleolus. You could then move it laterally by resecting tibial surface, and match it to the talus, and malunited piece. Alternatively, you could osteotomize the medial fragment, and debride the posterior piece, then move it laterally to meet the talus. I believe the syndesmosis should be stable, but be sure to stress it intra operatively. Hopefully the malunited pieces took enough plafond to keep the talus relatively congruent, and there don't appear to be any major step off's. There is some talus tilting at present. Let us know how it turns out.
James B. Carr, MD
Palmetto Health Orthopedics
Date: Tue, 21 Jan 2003 22:56:17 EST
From: Tadabq
The CT scan does seem to identify malunion of the distal tibia, although the exact detail of the fragments and their displacement is not perfectly clear. We think it would be an ideal case for a 3D model.
Tom DeCoster
George Brown
{kind=link}
{kind=link}
{kind=link}
{kind=link}